COVID-19 Pandemic: Nutritional Balance as Modifiable Risk Factor
On this page
Nutri-IQ™ is a unique tool that helps Wellness Professionals to identify nutritional gaps as COVID-19 modifiable risk factors. With deficiency in Zn, Vitamin A, C, D, B, immune system will not be able to protect from COVID-19!
Take a minute to review and find your vitamins deficiencies – they may be a root cause of your health problems and risks!
We already spoke about homeostasis as the dynamic state of equilibrium of a living organism. It would be logical to apply this concept to the threat ravaging the world when this post is being written, COVID-19.
Very serious scientists investigating importance of preventative nutritional approaches realized that nutritional imbalances do represent risks of getting sick with COVID-19. In this post, we provide a review of the latest scientific publications. Please let us know if you had seen any others, we would be happy to review them as well.
We have to note that medical community is mostly dealing with the disease when it takes moderate to severe course. In the contrary, community involved in nutritional research and application of nutritional principles is mostly focusing on evidence-based prevention techniques using the principles previously developed for other viral diseases.
Every day brings new observations, conclusions, and grim stats. Patients hospitalized with COVID-19 have received bills upward of $400,000. Unfortunately, human trials of susceptibility mitigation were not conducted, mostly because of ethical considerations, and suggested conclusions were based upon the following:
- observations;
- in-vitro research;
- animal studies.
All the research papers and systematic reviews mentioned here have extended lists of citations. They also agree that ethical controlled studies are required to confirm evidence-based suggestions and quantify the susceptibility risks. Until then, the recommendations of the reviews and citations they mentioned are mostly qualitative.
Immune Function Explained
The immune system role is to protect us from potential environmental dangers, including bacteria, viruses, fungi or parasites 1.
Our immune system is always active, but even more if we become infected. It responds to the threat depending on the invading pathogen type.
Viruses, including SARS-CoV-2 coronavirus causing COVID-19 disease, invade host cells. That can trigger presentation of antigens via MHC I, major histocompatibility complex molecules found on the cell surface on the surface of the infected cells1. Thus, infected cells are becoming antigens. Immune system response to virally infected cells works via recognition of the antigens by CD8+ cytotoxic T lymphocytes and natural killer cells. It results in killing the host cell that is presenting the antigen.
In general, the article1 describes human immune system as interdependency of the following functions:
- Creating a barrier to prevent pathogens from entering the body.
- Identifying pathogens if they breech a barrier.
- Eliminating pathogens.
- Generating an immunological memory.
These functions are explained in Appendix 1 in more detail.
Phases of COVID-19 Disease
COVID-19 goes through several phases. To recognize where we can modify the risk factors, we can have a look at the phases of COVID-19. The authors of 2 formalized COVID-19 phases as the following:
- Phase 1 – Prevention: in addition to regular preventative recommendations, the goal is “to support the patient in anticipation of the possibility that they’ll contract the virus”. The paramount is to activate and support immune system with proper nutrients.
- Phase 2 – Infection: supporting immune function to fight the infection.
- Phase 3 – Escalating inflammation: the key is to “stay away from manifesting the excessive inflammatory cytokine production and tissue destruction associated with sepsis”.
- Phase 4 – Recovery: the key is to down-regulate inflammation in order to avoid prolonged inflammatory and fibrotic effects
Authors of 2 noted that though inflammation activation is a very important component of the immune response, prolonged activation leads to the excessive lung damage according to the following model:
- Adequate activation > appropriate immune response > pathogen eradication & triggering of resolution phase chemistry > resolution
- Excessive activation > epithelial & endothelial tissue damage > DAMPs/PAMPs > further inflammatory cytokine generation > increased influx of immune elements (neutrophils, macrophages, etc.) > more damage > failure of resolution
Hence, the authors conclude that disease progression will depend on the degree of inflammation regulation during first and potentially second phases. Among other factors influencing level of inflammation during the the first phase, such as sufficient sleep, exercise, fresh air, and stress reduction, they mention proper diet ensuring sufficient level of certain nutrients in the body tissues.
Nutrients Affecting Disease Course
Let’s understand how nutrition affects course of COVID-19 disease.
Invading pathogens cause heightened activity of the immune system. Activation of the immune response induces the production of lipid-derived mediators such as prostaglandins and leukotrienes and of many different types of protein including immunoglobulins, chemokines, cytokines, cytokine receptors, adhesion molecules and acute-phase proteins. This requires availability of the substrate fatty acids and amino acids, respectively. The immune response involves significant cellular proliferation, so increasing the number of immune cells available for defence: this requires DNA, RNA, protein and complex lipid synthesis and the ready availability of substrates to support this.
The metabolic processes involved at heightened level of energy generation and biosynthesis require many different vitamins and minerals as cofactors1, 3.
Existing micronutrient deficiencies, even if only a single micronutrient, can impair immune function and increase susceptibility to infectious disease (Phase 1 support). Hence, optimization of overall nutritional status, including micronutrients, effective in reducing incidence of infectious disease, is beneficial as CPOVID-19 preventative measure 4.
Improvement of nutritional status (or, otherwise, one’s nutritional balance) can be performed either through the diet, or through supplementation, or through both. So, what nutrients could reduce the risk of getting sick5 or aggravating disease course6 for COVID-19? And what are the reasons for conclusions?
The following table adopted from 1 summarizes available today results of clinical trials and conclusions (mainly sourced from Cochrane database research). We can see that amount of trials is not sufficient to conclude definite correlation with COVID-19 prevention and outcomes. However, conducting on humans the randomized controlled trials for COVID-19 disease is clearly unethical and hence will not be performed int he near future. Thus, extending available results obtained for respiratory tract infections and pneumonia trials to forecast and mitigate COVID-19 disease risks seems viable.
| Micronutrient | Sample size | Main findings |
| Vitamin A 7 | 47 RCTs (1 223 856 children) | Vitamin A supplementation is associated with a clinically meaningful reduction in morbidity and mortality in children. |
| Vitamin A 8 | 15 RCTs (3021 children) | Vitamin A supplementation helps to relieve clinical symptoms and signs (of pneumonia) and shorten the length of hospital stay. |
| Vitamin C 9 | 3 prophylactic trials (2335 participants) two therapeutic trials (197 patients) | All three trials found vitamin C decreased the incidence of pneumonia. One trial found vitamin C decreased severity and mortality from pneumonia; the other trial found vitamin C shortened duration of pneumonia. |
| Vitamin C 10 | 29 prophylactic RCTs investigating incidence (11 306 participants) 31 prophylactic RCTs investigating duration (9745 episodes) | Vitamin C did not affect incidence of the common cold in the general population (24 RCTs) but decreased incidence in people under heavy short-term physical stress (5 RCTs). Vitamin C shortened duration of common cold in all studies (31 RCTs), in adults (13 RCTs) and in children (10 RCTs) and decreased severity of colds. |
| Vitamin D 11 | 11 RCTs (5660 participants) | Vitamin D has a positive effect against respiratory tract infections and dosing once daily seems most effective. |
| Vitamin D 12 | 25 RCTs (11 321 participants) | Vitamin D decreased the risk of acute respiratory tract infection, effects greater in those with low starting status |
| Vitamin D 13 | 24 studies; 14 included in meta-analysis of risk of acute respiratory tract infections and 5 in the meta-analysis of severity | There is an inverse non-linear association between 25-hydroxyvitamin D concentration and acute respiratory tract infection. |
| Vitamin D 14 | 8 observational studies (20 966 participants) | There is] an association between vitamin D deficiency and increased risk of community-acquired pneumonia. |
| Zinc, copper and iron 15 | 13 studies in Chinese children | The deficiency of zinc, copper and iron may be a contributing factor for the susceptibility of recurrent respiratory tract infection in children. |
| Zinc 16 | 7 RCTs (575 participants) | Zinc shortened duration of common cold. |
| Zinc 17 | 17 RCTs (2121 adults and children) | Oral zinc formulations may shorten the duration of symptoms of the common cold. |
| Zinc 18 | 6 RCTs (5193 children) | Zinc supplementation in children is associated with a reduction in the incidence and prevalence of pneumonia. |
| Zinc 19 | 6 RCTs (2216 adults with severe pneumonia) | Zinc given as an adjunct therapy decreased mortality. No effect of zinc on treatment failure or antibiotic treatment. |
- RCT=Randomized Controlled Trial
Vitamins
Vitamin A role
Vitamin A plays a role in the regulation of the innate immune response4 (through natural killer (NK) cells, macrophages and neutrophils) and cell-mediated immunity (through the growth and differentiation of B cells).
It is also active in humoral antibody immunity and in cytokine signalling, with a role in the inflammatory response as a result. First line of immune defence, skin and mucous membrane integrity, may be compromised in vitamin A deficiency. That leads to increased susceptibility to infection via the eyes, respiratory and gastrointestinal tract.
Hence, deficiency of Vitamin A causes increased vulnerability to infections such as measles, malaria and diarrhoeal diseases. Supplementation has been shown to be effective in all-cause mortality from infectious disease.
Based on these considerations, we decided to asses vitamin A deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
B-group vitamins role
According to 20, B vitamins are involved in intestinal immune regulation, thus contributing to gut barrier function.
According to 1, the following facts were observed in animal sudies:
- Folic acid deficiency in animals causes thymus and spleen atrophy, and decreases circulating T lymphocyte numbers.
- Spleen lymphocyte proliferation is also reduced.
- Vitamin B12 deficiency decreases phagocytic and bacterial killing capacity of neutrophils
- Vitamin B6 deficiency causes thymus and spleen atrophy, low blood T lymphocyte numbers and impaired lymphocyte proliferation and T lymphocyte-mediated immune responses.
- Vitamins B6 and B12 and folate all support the activity of natural killer cells and CD8+ cytotoxic T lymphocytes, effects which would be important in antiviral defence.
Patients with vitamin B12 deficiency had low blood numbers of CD8+ T lymphocytes and low natural killer cell activity. In a study in healthy older humans, a vitamin B6-deficient diet for 21 days resulted in a decreased percentage and total number of circulating lymphocytes, and a decrease in T and B lymphocyte proliferation and IL-2 production.
Repletion over 21 days using vitamin B6 at levels below those recommended did not return immune function to starting values, while repletion at the recommended intake (22.5 µg/kg body weight per day, which would be 1.575 mg/day in a 70 kg individual) did. Providing excess vitamin B6 (33.75 µg/kg body weight per day, which would be 2.362 mg/day in a 70 kg individual) for 4 days caused a further increase in lymphocyte proliferation and IL-2 production.
Consideration about niacin (vitamin B3) was provide in 21. The authors concluded that vitamin B3 helps to prevent inflammation damage associated with COVID-19.
Based on these considerations, we decided to asses B-group vitamins deficiencies (niacin, B6, B12 , folate) by Pandemic Risk Assessment Tool as COVID-19 risk factors.
Vitamin C role
Due to its ability to readily donate electrons, vitamin C is an effective antioxidant that enhances the activity and function of immune cells, white blood cell migration and leucocyte function via neutrophil and monocyte mobilization4 . It also has the potential to regenerate another antioxidant, vitamin E. Vitamin C increases epithelial barrier function and promotes oxygen radical scavenging activity of skin4 thus protecting the host from infection.
Deficiencies of vitamin C lead to impaired immunity and higher susceptibility to infection, increasing the risk of contracting pneumonia and also enhancing disease severity. The infection-related consequences of deficient vitamin C status are demonstrated clearly in chronic deficiency, otherwise known as scurvy, with pneumonia being one of the most frequent complications and causes of death. Infections, in turn, impact vitamin C stores due to enhanced inflammation and metabolic requirements, meaning the effects not mitigated at Phase 1 support can exacerbate and prolong the illness.
Dysfunctional epithelial barrier function of the lungs of animals can be restored by vitamin C administration. Supplementation is effective in both prevention and treatment of respiratory tract infections, having been shown to reduce incidence and duration of upper respiratory tract infection and severity of pneumonia in hospitalized older adults as well as symptoms of common cold. Prophylactic supplementation with vitamin C has also proven to reduce the risk of acquiring pneumonia, resulting in calls for intakes above RDA for the treatment of established infections, which require higher levels to compensate for the increased metabolic demand. Recent trial evidence, however, has demonstrated limited effects of high-dose supplementation on clinical endpoints in critically ill patients with acute respiratory distress syndrome.
Based on these considerations, we decided to asses vitamin C deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Vitamin D role
Observational data have suggested a strong relationship between low vitamin D status and the susceptibility to RTIs 22.
Vitamin D plays an important role in the innate immune system, through the production of antimicrobial peptides, including cathelicidin and defensins4.
Many cell types express vitamin D receptors, with particularly high levels existing in lung epithelial cells. Vitamin D depletion has the potential to increasing lung permeability and reducing pulmonary barrier integrity. The activation of vitamin D in the lung has the potential to induce these antimicrobials and attenuate inflammatory cytokines in response to viruses. Higher vitamin D status is associated
with decreased levels of proinflammatory cytokines and conversely low status appears to be associated with the activation of inflammatory processes, which is particularly relevant in the case of sepsis developed from lung infection.
Supplementation of vitamin D, particularly in those with lower baseline status, has proven effective in combating conditions like RTI, tuberculosis, chronic obstructive pulmonary disease, and asthma4. Meta analyses of randomised controlled trials (RCTs) presented above, have shown that vitamin D supplementation significantly reduces the incidence of RTIs, with baseline status and dosing frequency found to be independent modifiers of risk. Effects of supplementation were found to be strongest in those with baseline status <25 nmol/L and in groups who received daily supplementation or with higher baseline status4.
Based on these considerations, we decided to asses vitamin D deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Magnesium role (macromineral)
We have to note that magnesium is classified as a macromineral in the human body. However, its function affects a Vitamin (vitamin D), so we decided to keep them together.
A review 23 considered magnesium deficiency as a risk factor for COVID-19 since magnesium is involved in critical processes affected by COVID-19 disease. The author noted that hypokalemia appears to be a biomarker of imbalance as a common finding in patients with hypomagnesemia.
Magnesium role affects the following risk factors:
A. Subclinical magnesium deficiency is associated with an increase in low-grade chronic inflammation via endocrine disruptors, COVID-19 risk factor (experimentally induced magnesium deficiency in rodent models has been widely shown to elicit an inflammatory response).
B. Importance of vitamin D as anti-COVID-19 defence was discussed above. According to this publication, magnesium has ability to ability to activate and enhance the functionality of vitamin D. Several steps in vitamin D metabolism are dependent on magnesium as a cofactor, such as:
- Binding of vitamin D to vitamin D binding protein (VDBP)25(OH)D synthesis
- 1,25(OH)D synthesis
- 25-hydroxylase synthesis
- Vitamin D receptor (VDR) activation for cellular effects
Based on these considerations, we decided to asses magnesium deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Vitamin E role
Vitamin E is an antioxidant that protects the integrity of cell membranes from damage caused by free radicals. It has the potential to influence both innate and adaptive immunity4.
Alpha-tocopherol had shown to specifically enhance the dampened immune response associated with ageing.
Trial data on the effects of supplementation with vitamin E have been mixed, although has proven effective in reducing upper respiratory tract infections in elderly care home residents and improvements in innate natural killer cell response with supplementation 24
Based on these considerations, we decided to asses vitamin E deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Trace Elements
Zinc role
There is little zinc storage in the body. Thus, inadequate intakes can lead to deficiency associated with compromised immune function25, 26. In 27, the conclusion that frequently reported sudden worsening in COVID–19 disease could result from an abruptly depleted zinc–pool in already mild zinc deficient patients is presented.
Zinc is critical for the functioning of both innate and adaptive immunity, as well as cytokine production. It is altered during deficiency, contributing to oxidative stress and inflammation.This role in mediating inflammatory response is particularly relevant in the systemic inflammatory response observed in sepsis, an over-reactive host response to infection. Low zinc status has been associated with increased susceptibility to sepsis and fatality to infection.
According to 1, zinc inhibits the RNA polymerase required by RNA viruses, like coronaviruses, to replicate. That allows to suggest that zinc may play a key role in host defence against RNA viruses. In vitro replication of influenza virus was inhibited by the zinc ionophore pyrrolidine dithiocarbamate, and there are indications that zinc might inhibit replication of SARS-CoVs in vitro 28. In addition, the zinc-binding metallothioneins seem to play an important role in antiviral defence.
Zinc deficiency has a marked impact on bone marrow, decreasing the number immune precursor cells, with reduced output of naive B lymphocytes and causes thymic atrophy, reducing output of naive T lymphocytes. Therefore, zinc is important in maintaining T and B lymphocyte numbers.
Zinc deficiency impairs many aspects of innate immunity, including phagocytosis, respiratory burst and natural killer cell activity. Zinc also supports the release of neutrophil extracellular traps that capture microbes 29.
There are also marked effects of zinc deficiency on acquired immunity30. Circulating CD4+ T lymphocyte numbers and function (eg, IL-2 and IFN-γ production) are decreased and there is a disturbance in favour of T helper 2 cells 31. Likewise, B lymphocyte numbers and antibody production are decreased in zinc deficiency. Zinc supports proliferation of CD8+ cytotoxic T lymphocytes, key cells in antiviral defence.
Moderate or mild zinc deficiency or experimental zinc deficiency in humans result in decreased natural killer cell activity, T lymphocyte proliferation, IL-2 production and cell-mediated immune responses which can all be corrected by zinc repletion. In patients with zinc deficiency related to sickle cell disease, natural killer cell activity is decreased, but can be returned to normal by zinc supplementation32. Patients with the zinc malabsorption syndrome display severe immune impairments and increased susceptibility to bacterial, viral and fungal infections33.
Zinc supplementation (30 mg/day) increased T lymphocyte proliferation in elderly care home residents in the USA, an effect mainly due to an increase in numbers of T lymphocytes34.
The wide ranging impact of zinc deficiency on immune components is an important contributor to the increased susceptibility to infections, especially lower respiratory tract infection and diarrhoea, seen in zinc deficiency. Correcting zinc deficiency lowers the likelihood of diarrhoea and of respiratory and skin infections 1, although some studies fail to show benefit of zinc supplementation in respiratory disease.105 Meta-analysis of studies in Chinese children showed that those with recurrent respiratory tract infection were more likely to have low hair zinc. Recent systematic reviews and meta-analyses of trials with zinc report shorter duration of common cold in adults, reduced incidence and prevalence of pneumonia in children, and reduced mortality when given to adults with severe pneumonia (see references in the table above).
Based on these considerations, we decided to asses zinc deficiency by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Selenium role
Selenium influences the immune response largely through its action in selenoproteins, which function as cellular antioxidants.46 Deficiency appears to enhance virulence or progression of some viral infections 35 as evidenced by the relationship between Keshan disease, coxsackievirus B3 and influenza A, which are exacerbated by low selenium status. Selenium also has an important role in the modulation of the inflammatory response and cytokine
production.
Supplementation of selenium improves the immune system response to viruses in deficient individuals.Although scarce evidence of this has been demonstrated in humans, limited studies have shown functional outcomes of selenium supplementation on the human immune system. In one trial of UK adults with poor selenium status, supplementation with selenium attenuated poliovirus more rapidly than those given a placebo 36.
Caution is advised due to the adverse effects of selenium in high status and it is suggested those who are selenium sufficient should not supplement due to potential adverse effects. Selenium supplementation (100 to 300 µg/day depending on the study) has been shown to improve various aspects of immune function in humans37, including in the elderly. Selenium supplementation (50 or 100 µg/day) in adults in the UK with low selenium status improved some aspects of their immune response to a poliovirus vaccine.
Based on these considerations, we decided to asses selenium inadequacy by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Iron role
There are multiple reviews of studies of iron, immunity and infection. Iron deficiency induces thymus atrophy, reducing output of naive T lymphocytes, and has multiple effects on immune function in humans. The effects are wide ranging and include impairment of respiratory burst and bacterial killing, natural killer cell activity, T lymphocyte proliferation and production of T helper 1 cytokines. T lymphocyte proliferation was lower by 50% to 60% in iron-deficient than in iron-replete housebound older Canadian women 38.
However, there are also explanations for the detrimental effects of iron administration on infections and impairment of immune function39.
Based on these considerations, until positive role of iron is confirmed by the research community, we decided not to asses iron status by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Copper role
Copper deficiency in animals impairs a range of immune functions and increases susceptibility to bacterial and parasitic challenges. Human studies show that subjects on a low copper diet have decreased lymphocyte proliferation and IL-2 production, with copper administration reversing these effects40.
However, effect of of copper on respiratory diseases is mostly researched on animals. Copper as a risk factor for COVID-19 is still a hypothesis41. The authors agreed that despite of some evidence, more clinical studies are needed to draw a definite conclusion.
Based on these considerations, until positive role of copper is confirmed by appropriate studies, we decided not to asses copper status by Pandemic Risk Assessment Tool as COVID-19 risk factor.
Conclusion
Frequently, poor nutrient status is associated with inflammation and oxidative stress, which in turn can makes immune system incompetent. To achieve appropriate immune response, adequate and balanced supply of essential nutrients is required and needs to be monitored appropriately. There is so many signs and symptoms of nutritional imbalances that you can get lost and confused. Besides, optimal support of the immune system, depending on an adequate diet and nutrition in order to keep infection at bay in general population, especially under self-confinement, is challenging at the very least42.
No doubt, diet and nutrition influence the immune system competence and determine the risk and severity of infections43. There are bi-directional relationships between diet, nutrition, infection, and immunity. No doubt that the changes in one component have an impact on the others. The macro-, micronutrients, and phytonutrients in diet, mainly the fruits and colorful vegetables, generally promote healthy immune responses. These micro- and phytonutrients provide the antioxidants and the anti-inflammatory nutrients, including beta-carotene, vitamin C, vitamin E, which modulate the immune functions. The anti-inflammatory strategy, either by foods, nutrients, or medicines, is a viable option for COVID-19 management. Apart from the age-related micronutrient insufficiency, the nutritional status of an individual affects the risk of infection with SARS-CoV-II, the clinical course, and the outcomes of COVID-19. Therefore, the maintenance and monitoring of host macro- and micronutrient status is an important preventive measure for COVID-19.
Monitoring of the nutrients deficiency may seem like a cumbersome task for an average citizen. Luckily, there are Wellness Professionals who can use our tool, Nutri-IQ™ . It was built on the principles mentioned above using propriety Nutri-IQ technology assuming current RDAs.
Pandemic Risk Assessment Tool helps Wellness Professionals easily and conveniently identify clients’ nutritional gaps as possible disease risks. It allows to reveal and address the following deficiencies affecting immune function:
A. Vitamins
- Vitamin A
- B-group vitamins
- Vitamin C
- Vitamin D
- Vitamin E
B. Macrominerals
- Magnesium
C. Trace minerals
- Zinc
- Selenium
We can conclude that assessment of nutritional balance with Nutri–IQ™ is a cost-effective immediate measure for reducing a risk of getting sick with COVID-19.
Appendix 1: Immune System Functions
Barrier function
The barrier function of the immune system acts to prevent pathogens from entering the body from the external environment. This includes physical barriers like the skin and mucosal layers (gastrointestinal tract, respiratory tract, genitourinary tract); chemical barriers like the acid pH of the stomach; and biological barriers like the presence of commensal organisms on the skin and in the intestinal tract, secretions like IgA and antimicrobial proteins in saliva and tears, and the complement system.
Identification of pathogens
Pathogens are recognised by cells of the innate immune system, such as macrophages, monocytes and dendritic cells. This is achieved through the presence of pattern recognition receptors (PRRs) that recognize general molecular structures shared by groups of pathogens. These structures are called microbe-associated molecular patterns or MAMPs. When PRRs recognise MAMPs, the first line of host defensive responses is activated. PRRs include Toll-like receptors (TLRs). More than 10 functional TLRs have been identified in humans, each one detecting distinct MAMPs from bacteria, viruses, fungi and parasites.
Identification of pathogens
Pathogens are recognised by cells of the innate immune system, such as macrophages, monocytes and dendritic cells. This is achieved through the presence of pattern recognition receptors (PRRs) that recognize general molecular structures shared by groups of pathogens. These structures are called microbe-associated molecular patterns or MAMPs. When PRRs recognise MAMPs, the first line of host defensive responses is activated. PRRs include Toll-like receptors (TLRs). More than 10 functional TLRs have been identified in humans, each one detecting distinct MAMPs from bacteria, viruses, fungi and parasites.
Because viruses enter host cells, it is important that there are also exist intracellular TLRs that recognise viral DNA, viral double-stranded RNA and viral single-stranded RNA exist. Among these, TLR7 and TLR8 are found in macrophages, monocytes, dendritic cells and some other cell types and are likely to be important in innate recognition of the single-stranded RNA of coronaviruses. However, proteins, including the spike glycoprotein, of the coronavirus coat are also likely to be recognised by both intracellular and extracellular PRRs.
Elimination of pathogens
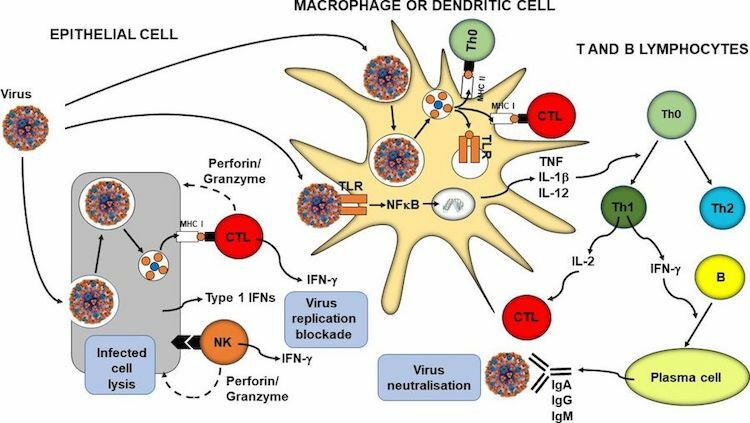
In parallel with phagocytosis, innate immune cell recognition of pathogens via PRRs triggers inflammatory signalling, activation of transcription factors like nuclear factor kappa-light-chain-enhancer of activated B cells (NFκB), inflammasome assembly, and production of classic inflammatory cytokines like tumour necrosis factor (TNF), IL-1β and IL-12. Viral infection of some cell types promotes release of type 1 IFNs (IFN-α and IFN-β) and these induce antiviral resistance, in part through activation of natural killer cells. Furthermore, virally infected cells directly activate natural killer cells which act to kill the infected cell. In addition, PRR signalling induces maturation of dendritic cells which are responsible for viral antigen processing and presentation, so initiating acquired immunity. Upregulation of MHC I on virally infected cells including both respiratory epithelial cells and dendritic cells results in presentation of viral antigens to CD8+ cytotoxic T lymphocytes. This activates them to kill virally infected cells through the release of pore forming proteins like perforin. Presentation of viral antigens via MHC II and the cytokines lead to the activation of CD4+ helper T lymphocytes with switching to the T helper 1 phenotype. These cells produce IL-2, which promotes cytotoxic T lymphocyte activity, and IFN-γ, which promotes differentiation of B lymphocytes to plasma cells which produce antiviral antibodies. These antibodies can bind to free viruses neutralising them. The processes involved in antiviral immunity are summarized below (sourced from 1 ).
Immunological memory
Immunological memory refers to the ability of the immune system to quickly and specifically recognize an antigen that the body has previously encountered and initiate a corresponding immune response.
- Antibodies can persist in the circulation for many months to many years, providing protection against reinfection.
- After the completion of disease course, a small number of memory T (both CD4+ and CD8+) and B lymphocytes remain. They are in a resting state but if they encounter the same antigen that triggered their formation they are able to respond immediately and lead to rapid elimination of the source of the antigen. Memory cells have a long life (up to several decades). Immunological memory is the basis of vaccination.
SARS-CoV-2 virus (the virus causing COVID-19 disease) is new to the human immune system and so there was no underlying existing natural immunity against it. SARS-CoV-2 infects respiratory epithelial cells and in severe cases requires ventilatory support.
References
- Calder PC: Nutrition, immunity and COVID-19 BMJ Nutrition, Prevention & Health 2020;3:doi: 10.1136/bmjnph-2020-000085
- Yanuck SF, Pizzorno J, Messier H, Fitzgerald KN. Evidence Supporting a Phased Immuno-physiological Approach to COVID-19 From Prevention Through Recovery. Integr Med (Encinitas). 2020;19(Suppl 1):8-35
- Lange, K. W., & Nakamura, Y. (2020). Food bioactives, micronutrients, immune function and COVID-19. Journal of Food Bioactives, 10. https://doi.org/10.31665/JFB.2020.10222
- McAuliffe S, Ray S, Fallon E, et al, Dietary micronutrients in the wake of COVID-19: an appraisal of evidence with a focus on high-risk groups and preventative healthcare. BMJ Nutrition, Prevention & Health 2020;bmjnph-2020-000100. doi: 10.1136/bmjnph-2020-000100
- Ranil Jayawardena, Piumika Sooriyaarachchi, Michail Chourdakis, Chandima Jeewandara, Priyanga Ranasinghe, Enhancing immunity in viral infections, with special emphasis on COVID-19: A review, Diabetes & Metabolic Syndrome: Clinical Research & Reviews, Volume 14, Issue 4, 2020, Pages 367-382, ISSN 1871-4021,https://doi.org/10.1016/j.dsx.2020.04.015
- Riccardo Caccialanza, Alessandro Laviano, Federica Lobascio, Elisabetta Montagna, Raffaele Bruno, Serena Ludovisi, Angelo Guido Corsico, Antonio Di Sabatino, Mirko Belliato, Monica Calvi, Isabella Iacona, Giuseppina Grugnetti, Elisa Bonadeo, Alba Muzzi, Emanuele Cereda, Early nutritional supplementation in non-critically ill patients hospitalized for the 2019 novel coronavirus disease (COVID-19): Rationale and feasibility of a shared pragmatic protocol, Nutrition, Volume 74, 2020, 110835, ISSN 0899-9007,https://doi.org/10.1016/j.nut.2020.110835
- Imdad A , Mayo-Wilson E , Herzer K , et al . Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst Rev 2017;3:CD008524. doi:10.1002/14651858.CD008524.pub3
- Hu N , QB L , Zou SY . Effect of vitamin A as an adjuvant therapy for pneumonia in children: a meta analysis. Zhongguo Dang Dai Er. Ke. Za Zhi 2018;20:146–53.
- Hemilä H , Louhiala P . Vitamin C for preventing and treating pneumonia. Cochrane Database Syst Rev 2013:CD005532. doi:10.1002/14651858.CD005532.pub3
- Hemilä H , Chalker E . Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev 2013:CD000980. doi:10.1002/14651858.CD000980.pub4
- Bergman P , Lindh Åsa U. , Björkhem-Bergman L , et al . Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PLoS One 2013;8:e65835
- Martineau AR , Jolliffe DA , Hooper RL , et al . Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ 2017;356:i6583.doi:10.1136/bmj.i6583
- Pham H , Rahman A , Majidi A , et al . Acute respiratory tract infection and 25-hydroxyvitamin D concentration: a systematic review and meta-analysis. Int J Environ Res Public Health 2019;16:3020. doi:10.3390/ijerph16173020
- Zhou YF , Luo BA , Qin LL . The association between vitamin D deficiency and community-acquired pneumonia: a meta-analysis of observational studies. Medicine 2019;98:17252
- Mao S , Zhang A , Huang S . Meta-Analysis of Zn, Cu and Fe in the hair of Chinese children with recurrent respiratory tract infection. Scand J Clin Lab Invest 2014;74:561–7.doi:10.3109/00365513.2014.921323
- Hemilä H . Zinc lozenges and the common cold: a meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage. JRSM Open 2017;8:205427041769429.doi:10.1177/2054270417694291
- Science M , Johnstone J , Roth DE , et al . Zinc for the treatment of the common cold: a systematic review and meta-analysis of randomized controlled trials. Can Med Assoc J 2012;184:E551–61.doi:10.1503/cmaj.111990
- Lassi ZS , Moin A , Bhutta ZA . Zinc supplementation for the prevention of pneumonia in children aged 2 months to 59 months. Cochrane Database Syst Rev 2016;12:CD005978. doi:10.1002/14651858.CD005978.pub3
- Wang L , Song Y . Efficacy of zinc given as an adjunct to the treatment of severe pneumonia: a meta-analysis of randomized, double-blind and placebo-controlled trials. Clin Respir J 2018;12:857–64.doi:10.1111/crj.12646
- Yoshii K , Hosomi K , Sawane K , et al . Metabolism of dietary and microbial vitamin B family in the regulation of host immunity. Front. Nutr. 2019;6:48.doi:10.3389/fnut.2019.00048
- Gebicki, J., Wieczorkowska, M. COVID-19 infection: mitohormetic concept of immune response. Cell Death Discov. 6, 60 (2020). https://doi.org/10.1038/s41420-020-00297-9
- Grant WB, Lahore H, McDonnell SL, et al. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients. 2020;12(4):988. Published 2020 Apr 2. doi:10.3390/nu12040988
- Taylor C. Wallace (2020) Combating COVID-19 and Building Immune Resilience: A Potential Role for Magnesium Nutrition?, Journal of the American College of Nutrition, DOI: 10.1080/07315724.2020.1785971
- De la Fuente M, Hernanz A, Guayerbas N, et al. Vitamin E ingestion improves several immune functions in elderly men and women. Free Radic Res 2008;42:272–80.
- Ander Mayor-Ibarguren, Carmen Busca-Arenzana, Ángel Robles-Marhuenda, A Hypothesis for the Possible Role of Zinc in the Immunological Pathways Related to COVID-19 Infection, Frontiers in Immunology, volume 11,p. 1736, 2020, doi: 10.3389/fimmu.2020.01736
- Mossink JP, Zinc as nutritional intervention and prevention measure for COVID–19 disease BMJ Nutrition, Prevention & Health 2020;3:doi: 10.1136/bmjnph-2020-000095
- Mossink JP, Zinc as nutritional intervention and prevention measure for COVID–19 disease BMJ Nutrition, Prevention & Health 2020;3:doi: 10.1136/bmjnph-2020-000095
- Uchide N , Ohyama K , Bessho T , et al . Effect of antioxidants on apoptosis induced by influenza virus infection: inhibition of viral gene replication and transcription with pyrrolidine dithiocarbamate. Antiviral Res 2002;56:207–17.doi:10.1016/S0166-3542(02)00109-2
- Subramanian Vignesh K , Deepe Jr. G . Metallothioneins: emerging modulators in immunity and infection. Int J Mol Sci 2017;18:2197. doi:10.3390/ijms18102197
- Hasan R , Rink L , Haase H . Zinc signals in neutrophil granulocytes are required for the formation of neutrophil extracellular traps. Innate Immun 2013;19:253–64.doi:10.1177/1753425912458815
- Ander Mayor-Ibarguren, Carmen Busca-Arenzana, Ángel Robles-Marhuenda, A Hypothesis for the Possible Role of Zinc in the Immunological Pathways Related to COVID-19 Infection, Frontiers in Immunology, volume=11, p. 1736, 2020, doi: 10.3389/fimmu.2020.01736
- Tapazoglou E , Prasad AS , Hill G , et al . Decreased natural killer cell activity in patients with zinc deficiency with sickle cell disease. J Lab Clin Med 1985;105:19–22.pmid:http://www.ncbi.nlm.nih.gov/pubmed/3968462
- Sandström B et al . Acrodermatitis enteropathica, zinc metabolism, copper status, and immune function. Arch Pediatr Adolesc Med 1994;148:980–5.doi:10.1001/archpedi.1994.02170090094017
- Barnett JB , Dao MC , Hamer DH , et al . Effect of zinc supplementation on serum zinc concentration and T cell proliferation in nursing home elderly: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr 2016;103:942–51.doi:10.3945/ajcn.115.115188
- Kiremidjian-Schumacher
L, Roy M, Glickman R, et al. Selenium and immunocompetence in patients with head and neck cancer. Biol Trace Elem Res 2000;73:97–112. - Broome CS, McArdle F, Kyle JAM, et al. An increase in selenium intake improves immune function and poliovirus handling in adults with marginal selenium status. Am J Clin Nutr 2004;80:154–62.
- Kiremidjian-Schumacher L , Roy M , Wishe HI , et al . Supplementation with selenium and human immune cell functions. II. Effect on cytotoxic lymphocytes and natural killer cells. Biol Trace Elem Res 1994;41:115–27.doi:10.1007/BF02917222 pmid:http://www.ncbi.nlm.nih.gov/pubmed/7946899
- Ahluwalia N , Sun J , Krause D , et al. Immune function is impaired in iron-deficient, homebound, older women. Am J Clin Nutr 2004;79:516–21.doi:10.1093/ajcn/79.3.516
- Weiss G . Iron and immunity: a double-edged sword. Eur J Clin Invest 2002;32 Suppl 1:70–8.doi:10.1046/j.1365-2362.2002.0320s1070.x pmid:http://www.ncbi.nlm.nih.gov/pubmed/11886435
- Hopkins RG , Failla ML . Copper deficiency reduces interleukin-2 (IL-2) production and IL-2 mRNA in human T-lymphocytes. J Nutr 1997;127:257–62.doi:10.1093/jn/127.2.257
- Syamal Raha, Rahul Mallick, Sanjay Basak, Asim K. Duttaroy, Is copper beneficial for COVID-19 patients?, Medical Hypotheses,Volume 142, 2020,109814,ISSN 0306-9877,https://doi.org/10.1016/j.mehy.2020.109814
- Iddir, M.; Brito, A.; Dingeo, G.; Fernandez Del Campo, S.S.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. https://doi.org/10.3390/nu12061562
- Amin Gasmi, Sadaf Noor, Torsak Tippairote, Maryam Dadar, Alain Menzel, Geir Bjørklund, Individual risk management strategy and potential therapeutic options for the COVID-19 pandemic,Clinical Immunology, Volume 215, 2020, 108409,ISSN 1521-6616, https://doi.org/10.1016/j.clim.2020.108409