
Magnesium: RDA, Dietary Sources, Deficiency Symptoms, and Functional Assessment
On this page
Abstract
In this article, we discuss the biological role of magnesium, the effects of magnesium deficiency, and current recommended dietary intakes:
- the major purposes of this specific nutrient in the human body,
- its experimentally confirmed health uses,
- conventional ways to estimate nutrient status,
- nutrient’s toxicities and deficiencies along with related symptoms,
- experimentally confirmed and approved levels of nutrient intake for different demographics,
- dietary sources of the nutrient.
Introduction
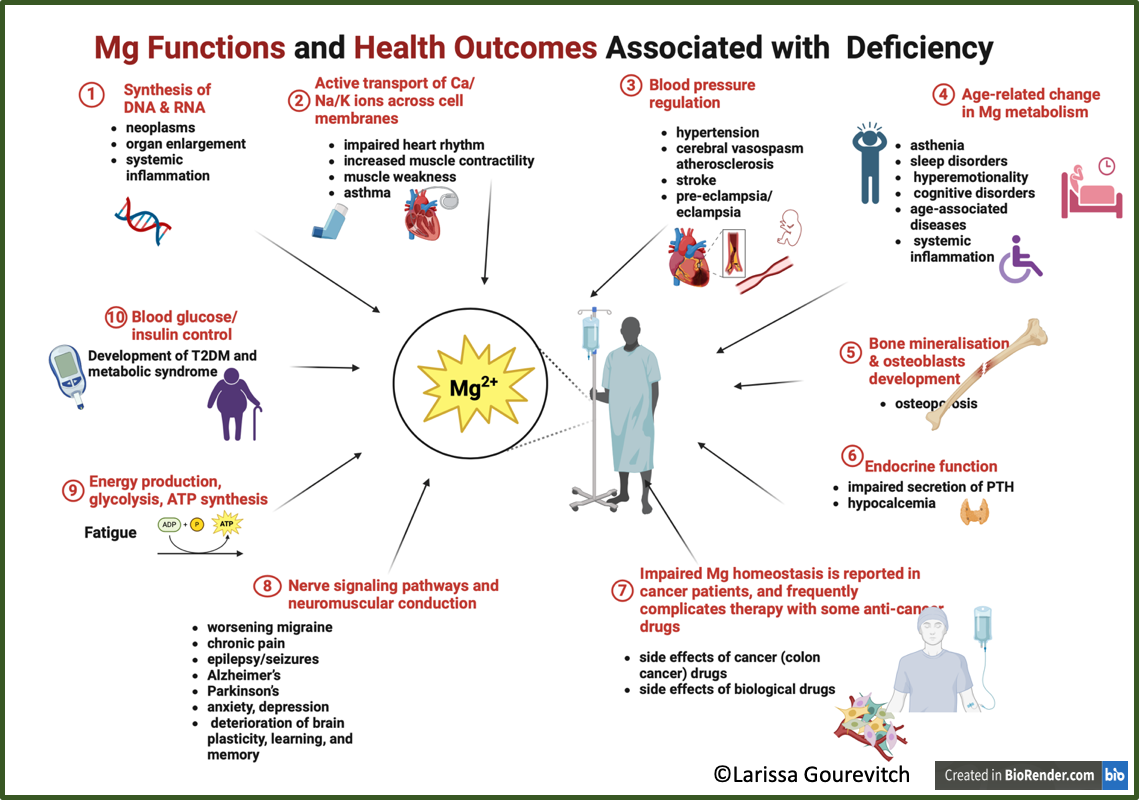
Magnesium, a mineral crucial for humans, is a cofactor in more than 600 enzyme systems that regulate diverse biochemical reactions in the body. That includes protein synthesis, muscle and nerve function, blood glucose control, and blood pressure regulation. Magnesium is required for energy production, oxidative phosphorylation, and glycolysis. It contributes to the structural development of bone and is required for the synthesis of DNA, RNA, and the antioxidant glutathione. Magnesium also plays a role in the active transport of calcium and potassium ions across cell membranes, a process that is important to nerve impulse conduction, muscle contraction, and normal heart rhythm.
Magnesium deficiency, even sub-clinical one, distorts these crucial biological processes.
Magnesium: Biological Functions and Importance of Homeostasis
Magnesium homeostasis is essential for a wide variety of metabolically important reactions4,6,9,32,45,23. Magnesium deficiency, hypomagnesemia, disrupts these reactions leading to undesirable health outcomes.
Among well-known functions of magnesium, the following are the most important:
- synthesis of DNA, RNA
- active transport of Ca/Na/K ions across cell membranes
- blood pressure regulation
- blood glucose/insulin control
- energy production, glycolysis, ATP synthesis
Emerging research also indicates the following biological functions:
- nerve signaling pathways and neuromuscular conduction
- aging
- oxygen uptake
- bone mineralization & osteoblasts development
- endocrine function
- immune function;
- co-factor in glutathione synthesis
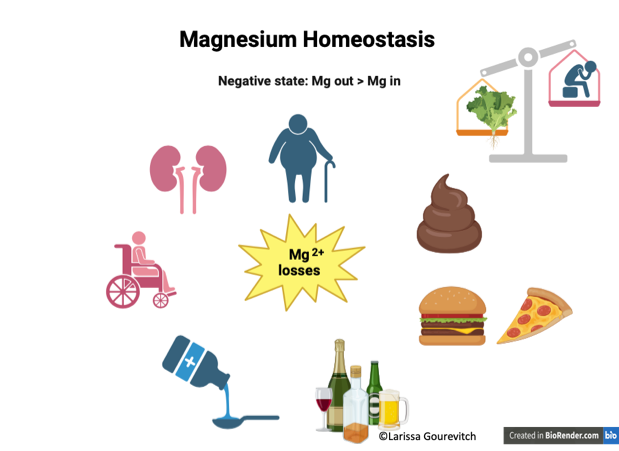
In a nutshell, magnesium homeostasis is regulated by the balance between intestinal absorption and renal excretion. Kidneys typically excrete about 120 mg of magnesium into the urine daily.
Magnesium’s role as a drug has been realized and more accepted recently. The following functions of magnesium enable its use as a therapeutic agent1,2,11,15,19,20,25,28,35,38,40:
- Natural calcium antagonist, vasodilator ⇨ hypertension, pre-eclampsia
- Glutamate NMDA receptor blocker ⇨ epilepsy; depression, anxiety, deterioration of brain plasticity, learning and memory; chronic fatigue; migraine
- Antioxidant, anti-inflammatory agent
- Promotes nerve regeneration after trauma
- Muscle relaxant
- Anticonvulsant/antipsychotic ⇨ epilepsy/seizures; Alzheimer’s, Parkinson’s, stroke; eclampsia)
- Painkiller ⇨ chronic pain
Symptomatic magnesium deficiency due to low dietary intake in otherwise healthy people is uncommon because the kidneys limit urinary excretion of this mineral. However, habitually low intakes or excessive losses of magnesium due to certain health conditions, chronic alcoholism, and/or the use of certain medications can lead to magnesium deficiency.
However, excessive magnesium content is also not benign, leading to some very unpleasant outcomes, such as
- diarrhea
- over-stimulation of the activity of osteoclasts and suppression of osteogenesis
- active tumour cells found to contain more Mg
Too much magnesium from food does not pose a health risk in healthy individuals because the kidneys eliminate excess amounts in the urine. However, high doses of magnesium from dietary supplements or medications often result in diarrhea that can be accompanied by nausea and abdominal cramping. Forms of magnesium most commonly reported to cause diarrhea include magnesium carbonate, chloride, gluconate, and oxide. The diarrhea and laxative effects of magnesium salts are due to the osmotic activity of unabsorbed salts in the intestine and colon and the stimulation of gastric motility.
Very large doses of magnesium-containing laxatives and antacids (typically providing more than 5,000 mg/day of magnesium) have been associated with fatal hypermagnesemia. The risk of magnesium toxicity increases with impaired renal function or kidney failure because the ability to remove excess magnesium is reduced or lost.
An adult body Mg content is 24–29 g. From that, 60% is contained in the bone; 20% – in skeletal muscle; 19% – in other soft tissues; and only 1% – in extracellular fluid (blood plasma & interstitial fluid).
Serum magnesium concentration is regulated by the balance between intestinal absorption and renal excretion
Habitually low intakes of magnesium induce changes in biochemical pathways that can increase the risk of illness over time.
Magnesium deficiency risks will be explored further.
Assessing Magnesium Status
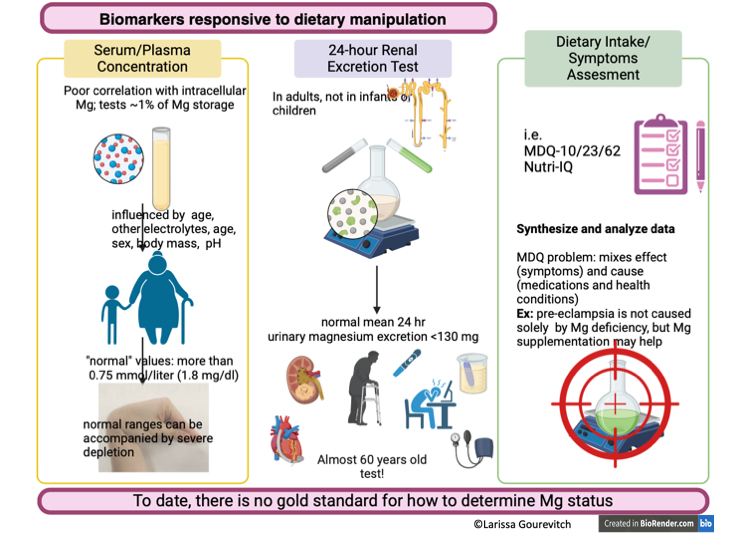
Assessing magnesium status is difficult because most magnesium is inside cells or in bone27,41,44. The most commonly used and readily available method for assessing magnesium status is the measurement of serum magnesium concentration, even though serum levels have little correlation with total body magnesium levels or concentrations in specific tissues. Other methods for assessing magnesium status include measuring magnesium concentrations in erythrocytes, saliva, and urine; measuring ionized magnesium concentrations in blood, plasma, or serum; and conducting a magnesium-loading (or “tolerance”) test. No single method is considered satisfactory. Some experts consider the tolerance test (in which urinary magnesium is measured after parenteral infusion of a dose of magnesium) to be the best method to assess magnesium status in adults. To comprehensively evaluate magnesium status, both laboratory tests and a clinical assessment might be required. That’s why magnesium status tests are not requested often.
Though clinical methods of magnesium status testing exist, the test is rarely requested in clinical settings. Officially, hypomagnesemia is defined as a serum magnesium level of less than 0.75 mmol/L. However, even normal serum magnesium concentrations ranging between 0.75 and 0.95 millimoles (mmol)/L may be associated with magnesium deficiency.
Urinary excretion is reduced when magnesium status is low. This fact is used as a baseline for another clinical test, urinary excretion.
Finally, magnesium status can be assessed via Nutritional Intake questionnaires. However, magnesium absorption rates vary from 30% to 60%.
The RDA for magnesium is quite high. To meet this, we need approximately 10 (!) cups of cooked spinach daily. Besides, current RDAs (see below) do not take into consideration differences in body weight in the same groups.
We have to conclude that, despite of existence a well-defined RDA, there is no gold standard for magnesium status assessments, though results of these tests may be responsive to dietary intake changes.
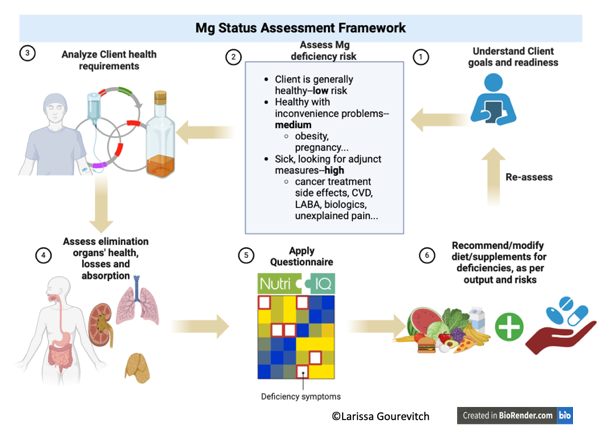
Functional Assessment of Magnesium Status
Instead of relying upon inconclusive tests, the Nutri-IQ team suggests starting with the functional assessment of Mg status. Nutri-IQ™ is a unique tool that enables feasible identification of clients’ nutritional gaps as possible causes for the complaints, such as feeling stressed, tired, depressed; insufficient effect of prescription medications with significant side effects, and inability to achieve optimal wellness, prevent chronic disease, and manage the aging process.
Then, dietary adjustment recommendations can be issued based on the unique client’s symptoms.
Let’s consider and evaluate the applicability of these symptoms in the case of magnesium.
Symptoms with Proven Causation to Magnesium Deficiency (Group A)
These Mg deficiency symptoms are confirmed by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes43:
- Hypocalcemia
- Impaired insulin secretion & insulin resistance
- Neuro-muscular hyperexcitability (spontaneous muscular activity such as cramps and spasms)
- Latent tetany signs:
- Chvostek’s sign (twitching of facial muscles in response to tapping over the facial nerve)
- Trousseau’s sign (carpopedal spasm, i.e. frequent and involuntary muscle contractions in the hands and feet with associated pain, induced by pressure applied to the arm, i.e. by blood pressure monitor or a ring)
That means that the symptom is uniquely identified with the fact of hypomagnesemia.
Symptoms Associated with Magnesium Deficiency
In certain circumstances, such as impaired renal excretion, a serious disease, or medications and treatments, magnesium homeostasis shifts towards imbalance, causing unpleasant but well-recognizable symptoms.
Emerging Research: Magnesium Deficiency Factors (Group B)
According to the latest research, the following symptoms (i.e. subjective client observations and complaints) are associated with hypomagnesemia1,4,5,10,11,14,15,26,28,32,33,38,40. Again, the studies showing a causation relationship are lacking as the relationship between symptoms and magnesium deficiency is not necessarily unique. For example, pre-eclampsia/eclampsia may be related to magnesium deficiency, but also may be caused by auto-immune factors.
- Chronic fatigue
- Tension-type headaches and migraines
- Stress
- Irritability, psychotic behaviour
- Mild anxiety/nervousness
- Aggression
- Tremors, convulsions, seizures
- Vertigo
- Confusion, disorientation
- Decrease in pain threshold
- Photosensitivity
- Tinnitus (ringing in the ears)
- Muscle weakness
- Gastrointestinal spasms
- Vomiting
- Nausea (also a symptom of Mg overdose)
- Mild sleep disorders
- Measurable signs:
- low potassium and calcium levels
- impaired parathyroid hormone release/function
- low potassium and calcium levels
- Vitamin D resistance (rickets requiring doses of vitamin D in excess of RDA)
- Calcification of soft tissue
- Cataracts
- Arrhythmias, tachycardia
Risk Factors for Excessive Magnesium Losses (Group C)
Among risks for magnesium deficiency, current research recognizes these factors leading to increased loss4,10,37,39:
- Gastrointestinal: Diarrhea, pancreatitis, irritable bowel disease, bowel resection, protein-calorie malnutrition, total parenteral nutrition, bowel fistula
- Renal: diuresis, tubular necrosis, renal transplantation, interstitial nephropathy
- Medications: Proton pump inhibitors, corticosteroids, laxatives, diuretics, antivirals, heart medications (digoxin), antifungals (amphotericin B), colchicines (anti-gout medications), theophylline (anti-asthmatic, anti-COPD), macrolide antibiotics, pentamidine (pneumonia drug), tobramycin (antibiotic for Gram-negative infections), amikacin (antibiotic for joint infections, intra-abdominal infections, meningitis, pneumonia, sepsis, and urinary tract infections), tacrolimus (immuno-suppressive drug); LABAs (long-lasting beta-antagonists for asthma treatment); aminoglycosides (Gram-negative antibacterial medications such as gentamicin, streptomycin);
- Chemotherapeutic/biologic agents: carboplatin, cisplatin (platinum chemotherapy); cetuximab (chemotherapy agent for colorectal, head and neck cancer); panitumumab (chemotherapy agent for colorectal cancer); cyclosporine (immunosuppressant); dupixent (biologic therapy; author’s assumption based on widely reported symptoms)
- Other: burns; alcoholism, post-op rehabilitation; excessive lactation
Diagnoses Associated with Magnesium Deficiency Symptoms (Group D)
Another set of factors are diagnoses associated with magnesium deficiency1,3,4,5,6,8,10,14,15,26,28,35,37,40,42,49. Causative effect though was not proved:
- Side effects of cancer and biological drugs
- Neoplasms
- Systemic inflammation, age-associated diseases
- CVD, mitral valve prolapse, hypertension, cerebral vasospasm, atherosclerosis, stroke
- T2DM/obesity/metabolic syndrome
- Fatigue, worsening migraine, asthenia, sleep disorders, hyperemotionality
- Chronic pain
- Epilepsy/seizures, Alzheimer’s, Parkinson’s
- Anxiety, depression
- Pre-eclampsia/eclampsia
- Asthma/COPD
- Osteoporosis, impaired secretion of PTH, hypocalcemia
- Primary hyperparathyroidism, hypoparathyroidism (hypercalciuria); hypercalcemia owing to overtreatment with vitamin D
- Primary aldosteronism
Understanding Magnesium Status
From the Functional Assessment standpoint, we recommend taking into consideration the association effect. In other words, we recommend offering adjunct measures, such as dietary intervention and/or Mg supplements, only if the client demonstrates symptoms from Group A, and/or symptoms from Group B accompanied by the risk factors from Group C and/or Group D

Magnesium Intake Recommendations
How much magnesium would prevent hypomagnesemia? The data below are provided based on decisions of the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes43.
Recommended by FDA Dietary Allowances (RDAs) for Magnesium
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months | 30 mg* | 30 mg* | ||
| 7–12 months | 75 mg* | 75 mg* | ||
| 1–3 years | 80 mg | 80 mg | ||
| 4–8 years | 130 mg | 130 mg | ||
| 9–13 years | 240 mg | 240 mg | ||
| 14–18 years | 410 mg | 360 mg | 400 mg | 360 mg |
| 19–30 years | 400 mg | 310 mg | 350 mg | 310 mg |
| 31–50 years | 420 mg | 320 mg | 360 mg | 320 mg |
| 51+ years | 420 mg | 320 mg |
*Adequate Intake (AI)
Based on the scientific research though this RDA needs to be increased by 25-50%4 bringing safe intake to about 500 mg/day.
The food content of magnesium is relatively low. To absorb RDA you would need to consume about 10 cups of cooked spinach! Our suggestion is to take into consideration whole-food magnesium (see below) and augment the amount with a good supplement. Our choice is the supplement with the optimal bioavailability from Seeking Health. Do not forget to claim your 10% discount with code IQ10!

Dietary Sources of Magnesium
Magnesium is widely distributed in plant and animal foods and in beverages. Green leafy vegetables, such as spinach, legumes, nuts, seeds, and whole grains, are good sources. In general, foods containing dietary fiber provide magnesium. Magnesium is also added to some breakfast cereals and other fortified foods. Some types of food processing, such as refining grains in ways that remove the nutrient-rich germ and bran, lower magnesium content substantially.
Tap, mineral, and bottled waters can also be sources of magnesium, but the amount of magnesium in water varies by source and brand (ranging from 1 mg/L to more than 120 mg/L).
Approximately 30% to 40% of the dietary magnesium consumed is typically absorbed by the body.
Selected Food Sources of Magnesium
| Food | Milligrams (mg) per serving | Percent DV* |
|---|---|---|
| Dry roasted almonds, 1 ounce | 80 | 19 |
| Boiled spinach, ½ cup | 78 | 19 |
| Dry roasted cashews, 1 ounce | 74 | 18 |
| Oil roasted peanuts, ¼ cup | 63 | 15 |
| Shredded wheat cereal, 2 large biscuits | 61 | 15 |
| Soymilk, 1 cup | 61 | 15 |
| Black beans, cooked, ½ cup | 60 | 14 |
| Cooked edamame, ½ cup | 50 | 12 |
| Smooth peanut butter, 2 tablespoons | 49 | 12 |
| Whole wheat bread, 2 slices | 46 | 11 |
| Avocado, cubed, 1 cup | 44 | 11 |
| Potato, baked with skin, 3.5 ounces | 43 | 10 |
| Brown rice, ½ cup | 42 | 10 |
| Plain yogurt, 8 ounces | 42 | 10 |
| Breakfast cereals, fortified with 10% of the DV for magnesium | 42 | 10 |
| Dark chocolate, 1 ounce | 41 | 10 |
| Instant oatmeal, 1 packet | 36 | 9 |
| Canned kidney beans, ½ cup | 35 | 8 |
| Banana, 1 medium | 32 | 8 |
| Cooked Atlantic salmon, farmed, 3 ounces | 26 | 6 |
| Milk, 1 cup | 24–27 | 6 |
| Halibut, 3 ounces | 24 | 6 |
| Raisins, ½ cup | 23 | 5 |
| Roasted chicken breast, 3 ounces | 22 | 6 |
| Pan broiled ground beef, 3 ounces | 20 | 5 |
| Broccoli, chopped and cooked, ½ cup | 12 | 3 |
| White rice, ½ cup | 10 | 3 |
| Apple, 1 medium | 9 | 2 |
| Raw carrot, 1 medium | 7 | 2 |
- *DV = Daily Value.
- The DV for magnesium used for the values in the table above is 420 mg for adults and children age 4 years and older.
- Foods providing 20% or more of the DV are considered to be high sources of a nutrient, but foods providing lower percentages of the DV also contribute to a healthful diet.
References
- Akarachkova, E. S. (2011). Chronic fatigue and approaches to its treatment. Neuroscience and Behavioral Physiology, 41(9), 899.
- Ashique, S., Kumar, S., Hussain, A. et al. A narrative review on the role of magnesium in immune regulation, inflammation, infectious diseases, and cancer. J Health Popul Nutr 42, 74 (2023). https://doi.org/10.1186/s41043-023-00423-0.
- Barbagallo M, Dominguez LJ. Magnesium and type 2 diabetes. World J Diabetes. 2015 Aug 25;6(10):1152-7. doi: 10.4239/wjd.v6.i10.1152. PMID: 26322160; PMCID: PMC4549665.
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. https://doi.org/10.3390/nu13020463.
- Castiglioni S, Cazzaniga A, Albisetti W, Maier JAM. Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions. Nutrients. 2013; 5(8):3022-3033. https://doi.org/10.3390/nu5083022.
- Castiglioni, S., & Maier, J. A. M. (2011). Magnesium and cancer: a dangerous liason. Magnesium Research, 24(3), 92–100. doi:10.1684/mrh.2011.0285
- Costello RB, Nielsen F (2017) Interpreting magnesium status to enhance clinical care: key indicators. Curr Opin Clin Nutr Metab Care 20:504–511
- Das SK, Haldar AK, Ghosh I, Saha SK, Das A, Biswas S. Serum magnesium and stable asthma: Is there a link? Lung India. 2010 Oct;27(4):205-8. doi: 10.4103/0970-2113.71944. PMID: 21139715; PMCID: PMC2988169.
- de Mier MVP-Ruiz, Santamarıa R, Peregrın CM, Gordillo JE, et al, Bone and vascular effects of magnesium supplements in CKD patients (the Magical Bone Pilot Study), NEFROLOG;A (2024), doi: https://doi.org/10.1016/j.nefro.2024.02.003.
- DiNicolantonio JJ, O’Keefe JH, Wilson W Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis Open Heart 2018;5:e000668. doi: 10.1136/openhrt-2017-000668
- Dominguez LJ, Veronese N, Barbagallo M. Magnesium and Hypertension in Old Age. Nutrients. 2021; 13(1):139. https://doi.org/10.3390/nu13010139.
- Drygała R, Waszczykowska K, Węgierska M. A summary of novel biologics for asthma treatment. Alergologia Polska – Polish Journal of Allergology. 2020;7(2):98-105. doi:10.5114/pja.2020.96130.
- Elin, R. J. (2010). Assessment of magnesium status for diagnosis and therapy. Magnesium research, 23(4), 194-198.
- Farhanghi MA, Mahboob S, Ostadrahimi A. Obesity induced magnesium deficiency can be treated by vitamin D supplementation. J Pak Med Assoc. 2009 Apr;59(4):258-61
- Fiorentini D, Cappadone C, Farruggia G, Prata C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients. 2021 Mar 30;13(4):1136. doi: 10.3390/nu13041136. PMID: 33808247; PMCID: PMC8065437.
- Forrest H Nielsen (2018) Magnesium deficiency and increased inflammation: current perspectives, Journal of Inflammation Research, 11:, 25-34, DOI: 10.2147/JIR.S136742
- Geiger, H., & Wanner, C. (2012). Magnesium in disease. Clinical kidney journal, 5(Suppl_1), i25-i38.
- Green, J., Valero, M., & Perkowski, L. (2015). Identifying and treating magnesium deficiency in cancer patients receiving platinum based chemotherapy. Natural Med J, 7.
- Hanada, T. Ionotropic Glutamate Receptors in Epilepsy: A Review Focusing on AMPA and NMDA Receptors. Biomolecules 2020, 10, 464. https://doi.org/10.3390/biom10030464
- Hou, H., Wang, L., Fu, T. et al. Magnesium Acts as a Second Messenger in the Regulation of NMDA Receptor-Mediated CREB Signaling in Neurons. Mol Neurobiol 57, 2539–2550 (2020). https://doi.org/10.1007/s12035-020-01871-z.
- https://www.mayoclinic.org/drugs-supplements/dupilumab-subcutaneous-route/ Drugs and Supplements: Dupilumab (Subcutaneous Route) Accessed on March 12, 2024
- https://www.mayoclinic.org/drugs-supplements/dupilumab-subcutaneous-route/side-effects/ Drugs and Supplements: Dupilumab – Side Effects Accessed on March 12, 2024
- J. Zhang, L. Tang, H. Qi, Q. Zhao, Y. Liu, Y. Zhang, Dual Function of Magnesium in Bone Biomineralization. Adv. Healthcare Mater. 2019, 8, 1901030. https://doi.org/10.1002/adhm.201901030.
- Kass, L. and Sullivan, K. (2016) Low Dietary Magnesium Intake and Hypertension. World Journal of Cardiovascular Diseases, 6, 447-457. doi: 10.4236/wjcd.2016.612048.
- Kim JY, Lee HJ, Lee HY, Lee S-M, Lee J, Park TY. The effects of hypomagnesemia on delirium in middle-aged and older adult patients admitted to medical intensive care units, The Korean Society of Critical Care Medicine 2586-6052, doi: 10.4266/acc.2022.00164
- Kirkland AE, Sarlo GL, Holton KF. The Role of Magnesium in Neurological Disorders. Nutrients. 2018 Jun 6;10(6):730. doi: 10.3390/nu10060730. PMID: 29882776; PMCID: PMC6024559.
- Magnesium deficiency. Accessed on March 12, 2024 at https://www.healthdirect.gov.au/magnesium-deficiency#symptoms
- Mathew, A.A., Panonnummal, R. ‘Magnesium’-the master cation-as a drug—possibilities and evidences. Biometals 34, 955–986 (2021). https://doi.org/10.1007/s10534-021-00328-7.
- Mills BJ, Lindeman RD, Lang CA. Magnesium Deficiency Inhibits Biosynthesis of Blood Glutathione and Tumor Growth in the Rat. Proceedings of the Society for Experimental Biology and Medicine. 1986;181(3):326-332. doi:10.3181/00379727-181-42260
- Muhammed, A. S., Abdullah Suhaimi, S. N., & Lee, Q. Z. (2021). Serum Magnesium: A Forgotten Electrolyte after Total Thyroidectomy. IIUM Medical Journal Malaysia, 20(3). https://doi.org/10.31436/imjm.v20i3.1700.
- Musso, C.G. Magnesium metabolism in health and disease. Int Urol Nephrol 41, 357–362 (2009). https://doi.org/10.1007/s11255-009-9548-7.
- National Institutes of Health, Office of Dietary Supplements Magnesium: Fact Sheet for Health Professionals. Accessed on March 8, 2024 https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional.
- Nielsen FH, Lukaski HC. Update on the relationship between magnesium and exercise. Magnesium research. 2006 Sep 1;19(3):180-9.
- Nielsen, F.H. The Problematic Use of Dietary Reference Intakes to Assess Magnesium Status and Clinical Importance. Biol Trace Elem Res 188, 52–59 (2019). https://doi.org/10.1007/s12011-018-1573-x.
- Nielsen, T.F., Rylander, R. Urinary calcium and magnesium excretion relates to increase in blood pressure during pregnancy. Arch Gynecol Obstet 283, 443–447 (2011). https://doi.org/10.1007/s00404-010-1371-y.
- Orlova S, Dikke G, Pickering G, Konchits S, Starostin K, Bevz A. Magnesium Deficiency Questionnaire: A New Non-Invasive Magnesium Deficiency Screening Tool Developed Using Real-World Data from Four Observational Studies. Nutrients. 2020 Jul 11;12(7):2062. doi: 10.3390/nu12072062.
- Pethő ÁG, Tapolyai M, Browne M, Fülöp T. Hypomagnesemia as a Risk Factor and Accelerator for Vascular Aging in Diabetes Mellitus and Chronic Kidney Disease. Metabolites. 2023; 13(2):306. https://doi.org/10.3390/metabo13020306.
- Pickering G, Mazur A, Trousselard M, Bienkowski P, Yaltsewa N, Amessou M, Noah L, Pouteau E. Magnesium Status and Stress: The Vicious Circle Concept Revisited. Nutrients. 2020; 12(12):3672. https://doi.org/10.3390/nu12123672.
- Rude RK, Singer FR & Gruber HE (2009) Skeletal and Hormonal Effects of Magnesium Deficiency, Journal of the American College of Nutrition, 28:2, 131-141, DOI: 10.1080/07315724.2009.10719764.
- Rosanoff A, Perspective: US Adult Magnesium Requirements Need Updating: Impacts of Rising Body Weights and Data-Derived Variance, Advances in Nutrition, 12, 2, 2021, 298-304, https://doi.org/10.1093/advances/nmaa140.
- Rude RK Chapter 24 – Magnesium Homeostasis, in Principles of Bone Biology (Third Edition), Academic Press, 2008, 487-513, https://doi.org/10.1016/B978-0-12-373884-4.00043-4.
- Singh JA, Wells GA, Christensen R, Tanjong Ghogomu E, Maxwell LJ, MacDonald JK, Filippini G, Skoetz N, Francis DK, Lopes LC, Guyatt GH, Schmitt J, La Mantia L, Weberschock T, Roos JF, Siebert H, Hershan S, Cameron C, Lunn MPT, Tugwell P, Buchbinder R. Adverse effects of biologics: a network meta‐analysis and Cochrane overview. Cochrane Database of Systematic Reviews 2011, Issue 2. Art. No.: CD008794. DOI: 10.1002/14651858.CD008794.pub2. Accessed 12 March 2024.
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. (1998). Dietary reference intakes: proposed definition and plan for review of dietary antioxidants and related compounds.
- Sutton RAL. Hypomagnesaemia and Magnesium Deficiency. J R Coll Physicians Lond. 1968 Jul;2(4):358-370. PMID: 30667743; PMCID: PMC5370652.
- Swaminathan R. Magnesium metabolism and its disorders. Clin Biochem Rev. 2003 May;24(2):47-66. PMID: 18568054; PMCID: PMC1855626.
- Volpe SL (2013) Magnesium in disease prevention and overall health. Adv Nutr 4:378S–383S
- Witkowski M, Hubert J, Mazur A. Methods of assessment of magnesium status in humans: a systematic review. Magnes Res. 2011 Dec;24(4):163-80. doi: 10.1684/mrh.2011.0292. PMID: 22064327.
- Wolf, F. I., Cittadini, A. R. M., & Maier, J. A. M. (2009). Magnesium and tumors: Ally or foe? Cancer Treatment Reviews, 35(4), 378–382. doi:10.1016/j.ctrv.2009.01.003
- Xue W, You J, Su Y, Wang Q. The Effect of Magnesium Deficiency on Neurological Disorders: A Narrative Review Article. Iran J Public Health. 2019 Mar;48(3):379-387. PMID: 31223564; PMCID: PMC6570791.
- Zhang J, Zhang B, Zhang J, Lin W, Zhang S. Magnesium Promotes the Regeneration of the Peripheral Nerve, Frontiers in Cell and Developmental Biology, 9, 2021, DOI=10.3389/fcell.2021.717854.
- Zieve FJ, Freude KA, Zieve L. Effects of magnesium deficiency on protein and nucleic acid synthesis in vivo. J Nutr. 1977 Dec;107(12):2178-88. doi: 10.1093/jn/107.12.2178. PMID: 925766.
- Elson Haas. “Staying Healthy with Nutrition”
Comments are closed.