
Histamine Intolerance: Am I Crazy or Allergic?
On this page
Nutri-IQ recommends to Wellness Practitioners the Histamine Intolerance Assessment Tool to check histamine intolerance as a possible cause of client’s complains. This article provides a snapshot of the evidence-based ways to recognize and manage histamine intolerance, and addresses its links to mental and gastrointestinal diseases.
Take a minute to review and find your vitamins deficiencies – they may be a root cause of your symptoms and intolerances!
Abstract
Whatever the reason is, the world is undergoing an epidemic of allergy and mysterious intolerances. In the western world, adverse reactions to ingested foods affect up to 20% of the population1 - cumulatively, this number is equal to the whole USA population2. Spread of mental illness is catastrophic - nearly 50% of the USA adults will develop at least one mental illness during their lifetime3. Inability to properly digest food is frightening: more than 40% of persons worldwide have functional gastrointestinal disorders, by the study of 33 countries on 6 continents4. And there is a hypothesis about an almost universal root cause for this avalanche of mysterious diseases: histamine intolerance. In this article, we will consider adverse systemic effects of excess histamine and its insufficient degradation, that is, histamine intolerance. We also will explain the role histamine plays in the body, and analyze its impact as physiological functions modulator. We also provide extensive bibliography of research and review scientific work covering these topics.
Histamine Role
Histamine is small organic molecule playing an important role in the body. It is known to be involved in 23 different physiological functions5. Among histamine physiological roles are:
- immune response to foreign pathogens,
- increase the permeability of the capillaries to white blood cells and some proteins, to allow them to affect pathogens in the infected tissues,
- local immune responses,
- inflammatory response,
- mediation of itching,
- regulation of digestion,
- vasodilation and blood pressure regulation,
- serving as a neurotransmitter for the brain, spinal cord, and uterus.
Histamine realizes its physiological functions via 4 receptors6. The receptors are extensively distributed within the body.
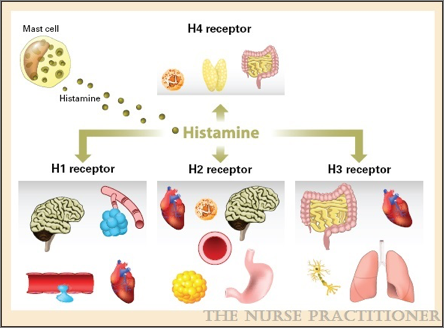
Due to the diversity of its physiological functions, histamine can be both a friend and a universal culprit with systemic effects.
Some health problems, such as high blood pressure, easily resolve by injecting of extra histamine7. Histamine’s actions are great for protecting the body against parasites8. But it also can be a ruthless killer. It is a common knowledge now that sudden histamine release resulting from COVID-19 cytokine storm can kill the host 9.
Our primary focus in this article is harmful effects of excess histamine in the body, that is, histamine intolerance.
What is Histamine Intolerance?
According to 10 “histamine intolerance, also referred to as enteral histaminosis or sensitivity to dietary histamine, is a disorder associated with an impaired ability to metabolize ingested histamine that was described at the beginning of the 21st century”.
Histamine intolerance is an indication that too much histamine is circulating in the body11. Histamine intolerance results from an excess of accumulated histamine and a lower capacity for histamine degradation. Obviously, the more unneeded histamine is imbalanced in the body, the more severe symptoms caused by the excess histamine may occur.
Most histamine in the body is preformed, stored in granules in mast cells and in basophils, released as needed, and then metabolized.
Excess of mast cell-derived histamine in circulation plays an important role in conditions associated with vascular leakage like urticaria and anaphylaxis, and is involved in other disorders, i.e. atopic dermatitis, asthma, and rheumatoid arthritis12. In food allergies it can cause vomiting and diarrhea.
Please note that despite of the substantial evidence accumulated about histamine metabolism, receptors, signal transmission, physiological and pathological effects, the complex interrelationships involving histamine yet remain to be understood13. And since this is an emerging topic, intolerance‐related physiological symptoms are not reliably treatable – yet.
Identification of Histamine Intolerance
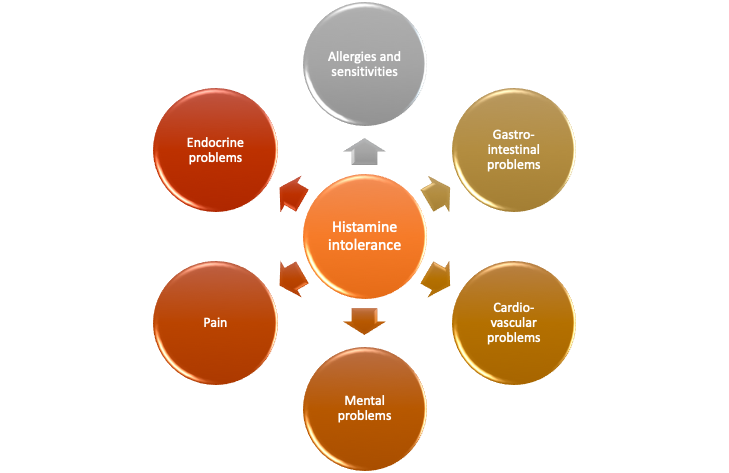
Diagnosis of histamine intolerance is difficult as clinical symptoms are often attributed to different diseases, such as allergy and food intolerance, or even mental disease. To commence differential diagnostics and assess probability of histamine intolerance as a possible root cause, several questionnaires analyze a given set of the symptoms14. Poly-intolerances/sensitivities are the most likely to be related to histamine intolerance15.
Nutri-IQ is offering to its subscribers convenient form of the questionnaire proposed and confirmed by Beverley Rider16. We have to note that evaluation of histamine intolerance assessment questionnaires is a popular research topic17! If histamine intolerance is likely, histamine ELISA (blood plasma histamine level) test can be ordered for the client. Blood allergy tests or skin testing will not be positive since histamine intolerance is not mediated by IgE antibodies.
Histamine Sources and Degradation
There are endogenous (internal) and exogenous (external) sources of histamine that can lead to histamine intolerance18. The article points out to the following sources of histamine:
Endogenous sources of histamine:
- gastric enterochromaffin cells,
- histaminergic neurons,
- mast cells and basophils which store histamine in intracellular vesicles release histamine upon stimulation by non-immune, chemical, and physical factors:
- neuropeptides (substance P),
- parts of complement system,
- immunity and inflammation mediators cytokines (IL-1, IL-3, IL-8, and GM-CSF),
- platelet activating factor (PAF),
- hyperosmolarity (high concentration sodium or glucose in the blood),
- lipoproteins (cholesterol),
- adenosine and some other medications,
- enzymes, i.e. superoxidases,
- hypoxia,
- extreme temperatures,
- stress and trauma via corticotropin-releasing factor sending signals to mast cells to release histamine19,
- vibrations,
- alcohol,
- some certain types of food.
Exogenous sources of histamine:
- ingestion of high-histamine foods (due to thermostability, histamine which is present in food is almost irremovable), i.e. fermented foods, beer, wine, cheeses, meat, soy, yogurt,
- microbial decarboxylation of histidine by different fermenting bacteria, including natural human flora in the gut.
Histamine degradation:
Histamine is metabolized extracellularly by diamine oxidase (DAO), or intracellularly by histamine-N-methyltransferase (HNMT)20.
Please note that for proper functioning of DAO enzyme, it needs cofactors: vitamins B6 and C, and copper21. Nutrition competency regarding these cofactors can be checked using Nutri-IQ Nutritional Balance Assessment Tool. DAO can be inhibited by some medications, such as chloroquine, clavulanic acid, Cimetidine, verapamil, isoniazid, metamizole, acetyl cysteine, amitriptyline, diclofenac, metoclopramide, suxamethonium, thiamine (vitamin B1)22.
Blending into the Crowd
Further in this article, we will consider how histamine intolerance blends with other health issues. Keep in mind that addressing the root cause, histamine intolerance, will almost instantly alleviate related issues!
Allergy, Food Sensitivity, and Histamine Intolerance
In allergies and food sensitivities, the immune system overreacts to harmless substances instead of invaders. It is easy to distinguish “classic” allergy from food sensitivity by the mediation type (IgG vs IgE antibodies 23 ), and the fact that sensitivities do not cause anaphylactic shock reaction. The number of people affected by these problems is equal to the whole USA population!
The clinical expression of allergic diseases depends on the actions of several mediators. Histamine, as it was recognized and studied since 1911, is prominent among them24. Histamine mediates the following symptoms in anaphylaxis and allergic responses of the skin, nose, and airways:
- bronchospasm, edema , and mucus secretion in asthma,
- pruritus, mucosal edema and secretion, sneezing in allergic rhinitis,
- urticaria (vasodilation, vascular permeability, and pruritus) in the skin reactions,
- vascular permeability, smooth muscle contraction, mucus secretion and tachycardia in anaphylaxis.
Excess histamine may exacerbate the above symptoms as an uncontrolled process mediator. Thus, it becomes the foe.
If histamine intolerance is suspected, lab tests of the histamine plasma levels can be performed. Levels above >10 nmol/L correlate with severe allergic response25. Plasma histamine levels of the subjects with suspected histamine intolerance is usually higher that for those with food allergy26.
The most typical among the histamine intolerance symptoms are27:
| System | Histamine Intolerance Symptom |
| All systems involved | Body temperature rising |
| Cardio-vascular | Hypotension and tachycardia |
| Gastro-intestinal | Heartburn – due to increased acid production Abdominal pain Diarrhea Vomiting |
| Respiratory | Anaphylaxis Bronchial asthma Nasal congestion, rhinorrhea, sneezing, nose and throat itching Bronchial obstruction |
| Nervous system | Headaches |
| Integumentary | Skin pruritus (itch) Urticaria (hives)+eczema sometimes called histamine rash Angioedema (swelling of face/hands/lips) Erythema (redness of the skin or mucous membranes caused by increased blood flow) |
| Vision | Ocular itch/burning |
| Endocrine system | PMS – histamine-induced contractions due to hormone levels changes |
These are very unpleasant symptoms. However – and this is good news – if histamine intolerance is suspected and confirmed, there are tools to mitigate these effects. Nutri-IQ questionnaire helps to identify the probability that systemic symptoms affecting your client in fact relate to histamine intolerance.
Further, we will provide some insights on how histamine intolerance is involved with nervous and gastroenterological problems that are rarely suspected to be affected by histamine excess.
Histamine Role for Nervous System
Histamine is a central nervous system neurotransmitter and neuromodulator. The histaminergic system in the human brain is really extensive (approximately 64,000 neurones)28.
Histamine is necessary to maintain wakefulness, alertness, and reaction time29. Also, histamine contributes to modulation of circadian rhythms, homeostasis, motor behaviour, and cognition30,31.
Evidence suggests that histamine intolerance may play an important role in the pathophysiology of some nervous system diseases, such as anxiety, depression, psychosis, stroke, Alzheimer’s disease, Parkinson’s disease, attention-deficit hyperactivity disorder, migraine, epilepsy, vascular dementia, mental retardation, cerebrovascular encephalopathy, multiple sclerosis, brain tumors, cranial nerve neuropathies, mental retardation and post-traumatic brain injury32, 33.
Depression. Though it was not tested on humans, blocking histamine receptor in the brain (H3 receptor) alleviated depression-like state34!
Insomnia. Short-term insomnia can be treated with antihistamines35. The effect is related to antagonizing H1 receptors in tuberomammillary nucleus and inhibiting the arousal pathways.
Epilepsy: A cohort study found that children with allergic rhinitis (characterized by spontaneous degranulation of mast cells and release of histamine) have a 76 % increased subsequent risk of epilepsy36.
Addictions: Review 37 confirmed amplification effect that histamine exerts on later stages of addictive and over-consuming behaviours, when drug/food intake is driven by habit.
Pain. Worldwide prevalence rate of neuropathic pain in the general population lies between 7% and 10% 38. Histamine is an excitatory neurotransmitter generating pain hypersensitivity. Inhibition of histamine receptor signalling causes neuroprotective and antinociceptive effects39. Pain‐modulatory effects of histamine depend on the amount of histamine administered/circulating40. The studies support the idea that H1 and H2 receptor antagonists permeable into the central nervous system may potentially be used as analgesics for patients with neuropathic pain41.
Observational study of patients with severe pelvic pain due to endometriosis42 had shown statistically higher histamine intolerance levels (histamine level in peripheral blood), along with higher depression and anxiety levels.
Autism Spectrum Disorders (ASD): Another “epidemic” is proliferation of autism spectrum disorders43. The article estimates prevalence of ASD in western countries as high as 11 cases per 1000! According to44, histamine from brain mast cells may be involved in the ASD pathogenesis and can worsen symptoms with stress.
Histamine Intolerance and GI Tract
In the GI tract, histamine is synthesized by histidine decarboxylase (HDC) enzyme and stored in various cell types. They release histamine following activation by allergens or mitogens (peptides that induce cell division) or cytokines45.
Functional GI disorders are characterised by chronic complaints regarding dysmotility and hypersensitivity. These complaints arise from disorganised brain–gut interactions. Functional dyspepsia and IBS (irritable bowel syndrome) are the two most prevalent FGIDs, affecting up to 16–26% of worldwide population46. In turn, the study47 confirmed that gut mucosa and supernatant of patients with IBS contain increased concentrations of histamine.
Multiple studies confirmed successful application of antihistamine medication to alleviate IBS48. Pain is the major inconvenience of IBS, and histamine was confirmed as IBS pain exacerbating factor.
In another study49, histamine intolerance, that was found in more than 50% of participants with non-responsive celiac disease, was identified to play an important role in disease course.
The most recent gastroenterology recommendation is to consider histamine intolerance in the differential diagnoses of patients with functional, nonspecific, non-allergic gastrointestinal complaints50.
Addressing Histamine Intolerance
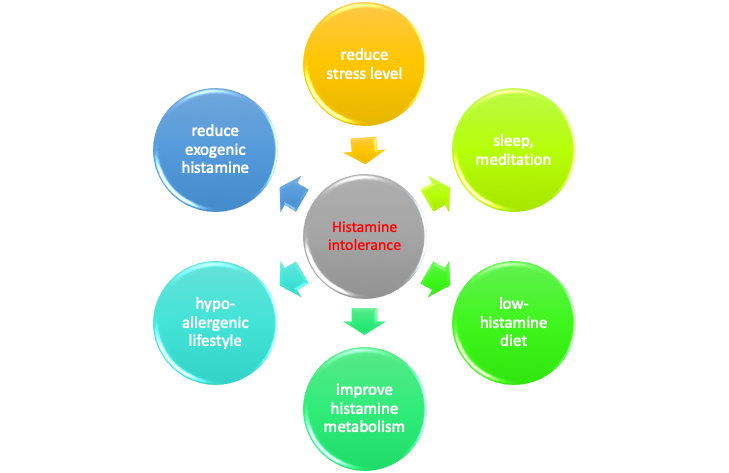
Based on the histamine balancing mechanism, unpleasant effects of histamine intolerance may be lessened if amount of histamine circulating in the body is reduced, or if the body improves its ability to metabolize histamine. Our body does not distinguish between endogenous (released by the body) and exogenous (coming with food or released by intestinal bacteria) histamine. So, very often there is a mentioning of a “bucket”, that is, a cumulative histamine load in the body. Thus, to deal with the problem and “empty the bucket”, one can:
- Reduce amount of endogenous and exogenous histamine released and circulating in the blood and digestive system by:
- reduction of stress level, sleep hygiene, meditation,
- exclusion from the diet foods high in histamine,
- supporting “good” bacterial in the gut that either do not release histamine, or help to metabolize it,
- adoption of hypoallergenic life-style,
- taking correct type of anti-histamine medication.
- Improve metabolism of histamine already released or consumed and circulating int he body by:
- nutritional support of histamine-metabolizing enzymes,
- correct type of medication improving histamine metabolism.
We will consider rationale of those measures further in this article.
Addressing Stress Levels
As it was mentioned before, stress and anxiety increase histamine release from cells.
A study determined how steady-state plasma histamine levels are regulated and affected by environmental factors51. Since 1960-s, circadian variations of plasma histamine levels, with increase in the early morning hours, were documented. These nocturnal peaks in plasma histamine levels are implicated in the nighttime exacerbation of asthma symptoms. The article concluded that the mast cell “clock” mediates circadian release of histamine! The stress negative effect is that it deregulates mast cell “clock” leading to spontaneous release of histamine in arbitrary hours. The type of stress my be sub-acute, or interchange of light and ark conditions.
That’s why we conclude that in order to take control of histamine intolerance, it is important to manage stress levels by focusing on good sleep, breathing and diet.
Histamine-Friendly Nutrition
Currently, international health administrations consider histamine intoxication to be one of the main problems of global food security, due to both for its effects on human health and its impact on trade52. The foods with high concentrations of histamine can be a risk to consumers, especially in individuals taking drugs that inhibit DAO or MAO as well as in patients with mastocytosis, tumor, or chronic myelocytic leukemia.
One of the pathways is the ingestion of histamine-rich food, alcohol, or drugs that release histamine. They may provoke diarrhea, headache, rhinoconjunctival symptoms, asthma, hypotension, arrhythmia, urticaria, pruritus, flushing, and other conditions in patients with histamine intolerance53. Approximately 1% of the population has histamine intolerance.
Histamine-friendly nutrition is based on 2 principles:
- reduce amount of histamine coming with foods;
- improve action of histamine-metabolizing enzymes.
Reducing Histamine Load
In the study54, a total of 75% of the patients had improvement of histamine-intolerance symptoms from the low‐histamine diet. It also was demonstrated that lower-histamine diet improves histamine intolerance symptoms and causes an increase in serum DAO values55. The website Healing Histamine provides nice and non-restrictive ways to create histamine-friendly nutrition.
So, if histamine intolerance is suspected, the logical way is to reduce dietary histamine load. App stores have Food Intolerances apps that are a bit costly though. As we are not paid to provide advertisement, we won’t! But it always makes sense to check recipes for the histamine content.
Unfortunately, there are no clear guidelines on how much histamine in the food is safe for allergic consumers. Since there is no baseline, we would recommend to check histamine-friendly food list here.
There are sufficient research data estimating absolute value of dietary histamine content, and effects of the food preparation and storage. Below, we collected some data that can be used comparing other meal options. Foods of animal origin (meat, fish, eggs, dairy) usually contain higher histamine content56:
| Food | Histamine content (mg/kg) in some food of animal origin and wine (mg/l) |
| Fish | |
| Indian mackerel | 13.0 |
| Fresh anchovies | 69.0 |
| Fresh sardines | 62.0 |
| Fresh tuna | 478.0 |
| Tuna hamburger | 304.0 |
| Oil-preserved mackerel | >720.0 |
| Salted mackerel | 68.0 |
| Salted tuna | 146.0 |
| Cheese | |
| Parmigiano Reggiano | 38.4 |
| Grana Padano | 23.9 |
| Provolone Valpadana | 9.7 |
| Pecorino Crotonese | 19.1 |
| Caciocavallo Silano | 42.0 |
| Cabrales blue | 957.6 |
| Gouda | 40.0 |
| Gorgonzola | 255.3 |
| Roquefort | 376.6 |
| Fermented sausages | |
| Catalao | 6.1 |
| Salsichao | 12.5 |
| Salami | 192.0 |
| German types | 6.2 |
| French types | 2.3 |
| Italian types | 1.4 |
| Wine | |
| Red | 25.1 |
| White | 12.5 |
| Rose | 13.4 |
The same source provides data that foods of vegetable origin usually have lower histamine content:
| Food | Histamine content (mg/kg) in food of vegetable origin |
| Soy sauce | nd-592 |
| Sufu | 730.0 |
| Miso | nd-221 |
| Natto | nd-457.0 |
| Soy milk | 17.5 |
| Tempeh | 4.1 |
| Tofu | 3.5–5.8 |
| Soybean paste | 51.2 |
| Tamari | 57.65 |
| Tomato pasta | 2.0–10.1 |
| Ketchup | 2.0–18.0 |
| Spinach puree | 2.1–9.8 |
| Green pea | 2.3–3.8 |
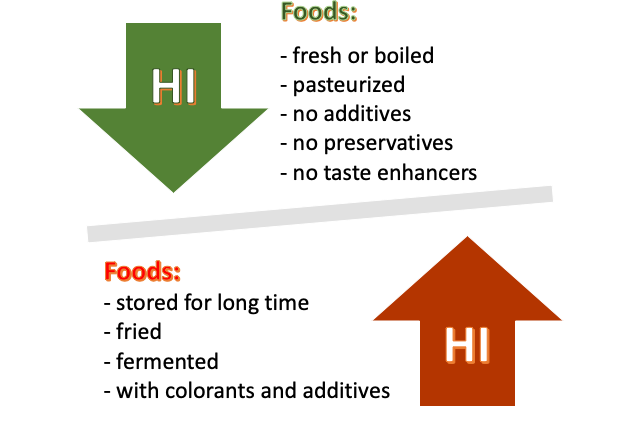
Food’s histamine load can be increased by the duration of storage, preparation method, and additives57.
Improving Histamine Metabolism
Some research suggests that an adequate intake of healthy fats and other nutrients — like phosphorus, zinc, magnesium, iron, and vitamin B12 — may play a role in enhancing DAO activity58. Deficiency in these important nutrients can be assessed virtually using Nutri-IQ Nutritional Balance Assessment Tool.
DAO production can also be improved nutritionally. Enzymatic activity of histidine DAO can last even after bacterial autolysis.
There are common foods that inhibit histamine metabolism. When intolerance is suspected, they may be eliminated from the diet or limited. According to 59, foods that may interfere with DAO and HMNT levels or actions include:
- alcohol
- energy drinks
- green tea
- black tea
- mate tea
- raw egg whites
- some yogurt, depending on bacteria type
We have seen multiple complains from the clients when the cleanest diet brought just borderline effect. In those cases, lifestyle changes are the must, and intervention with antihistamines or other medications is required.
Reduction of Exogenous Histamine
World Health Organization (WHO) defines probiotics as “live microorganisms which confer a health benefit on the host when administered in adequate amounts”60. Exogenous histamine released by intestinal bacteria (probiotic bacteria) is a very important component of the “histamine bucket” and hypersensitivity responses.
In terms of histamine, probiotic bacteria can be61:
- Releasing histamine or suppressing DAO production:
- certain gram-negative bacteria such as Escherichia coli and Salmonella typhimurium,
- Lactobacillus casei and Lactobacillus bulgaricus (though not all strains within these species will have this effect, but if in doubt then avoid these species to be sure).
- Neutral in terms of histamine and/or DAO production:
- Lactobacillus acidophilus NCFM®,
- Bifidobacterium lactis BI-04®,
- B. lactis HN019.
- Suppressing histamine and supporting DAO production:
- Lactobacillus paracasei CASEI 431® (not to be confused with Lactobacillus casei as they are completely different species),
- Lactobacillus rhamnosus,
- Bifidobacterium infantis,
- Bifidobacterium longum,
- Lactobacillus plantarum,
- (possibly) Lactobacillus reuteri,
- Lactobacillus plantarum D-1033,
- Lactobacillus rhamnosus GG®.
The following schematics explaining mechanics of probiotics action was adopted from62:

Addressing Histamine Intolerance with Medications
Anti-histamine medications represent first line of defence to reduce severity of histamine intolerance. Antihistamines block the binding of histamine to its receptors or reduce histamine receptor activity63, acting as receptor antagonists.
Pharmacological Antihistamines
Antihistamine medications are selected and prescribed based on physiological function64. They affect histamine receptors responsible for the onset of uncomfortable symptoms. Depending on the symptom severity, anti-histamine medications may be either available by prescription only or sold over-the-counter.
Please note that H1 antihistamine medications can cross the blood–brain barrier and cause some detrimental effects on the (CNS), such as hangover-like effects, concentration lapses, lower learning ability65.
| Physiological function of histamine receptors | Antihistamine medication | |
| H1 histamine receptor •Present in CNS, smooth muscle, heart, immune, epithelial, endothelial, adrenal, and sensory nerve cells •Mediates post-synaptic effects of histamine in CNS •Stimulates smooth muscle contraction in GI and respiratory tract •Stimulates sensory nerves causing itching, sneezing, and edema | First generation: •Chlorpheniramine •Clemastine •Diphenhydramine •Hydroxyzine | Second generation •Cetirizine •Fexofenadine •Levocetirizine •Loratadine |
| H2 histamine receptor •Found in gastric mucosa, heart, CNS, immune, airway smooth muscle, endothelial, and uterine cells •Mediates parietal cells gastric secretion •Relaxes smooth muscles and airway vascular system •Increases heart rate and contractility | •Cimetidine •Famotidine •Ranitidine •Nizatidine | |
| H3 histamine receptor •Found primarily in CNS •Conducts pre-synaptic regulation of neurotransmitters (dopamine, norepinephrine), serotonin, acetylcholine, and histamine) •Relaxes smooth muscles in airways | •Ciproxifan •Pitolisant | |
| H4 histamine receptor •Found in bone marrow, blood, spleen, thymus, lung, GI tract, and CNS •Mediates Ca function in mast cells •Mediates mast cell migration | •Alcaftadine |
Nutraceutical Antihistamines
Just a small number of herbs had been studied to provide antihistamine effects, and corresponding supplements sold by a Health Food store can assist with root causes and effects of histamine intolerance.
Mast cells can actually be stabilized by several botanicals. A special place belongs to Quercitine as an effective histamine release blocker66. In supplement formulas, it is sometimes mixed with bromelain to reduce inflammation. Also, prickly pear (Opuntia elatior) had shown to reduce mast cell degranulation67.
For almost 60 years, FDA-approved antihistamine Cromolyn sodium is a golden standard of prevention of mast cell degranulation68. It was initially extracted form plant khella (Ammi visnaga) which had been used as a muscle relaxant since ancient times in Egypt and afterwards was synthesized chemically69. Please note that some preparations of Cromolyn Sodium are sold bye prescription only.
Interesting research is described in 70 suggested that administration of activated charcoal may be useful to prevent further absorption of peanut protein from the GI tract and avoid excessive release of histamine, after accidental ingestion by individuals with peanut allergy.
Other botanicals with antihistamine properties include:
- Widely researched is Astragalus membranaceus (also known as Astragalus, Huáng qí or Milkvetch). It possesses immunoregulatory functions of allergic diseases and can be used as an inflammatory component of allergic asthma treatment71.
- Perilla seeds are a good source of polyunsaturated fatty acids. They suppress the production of chemical mediators in the allergy and inflammatory responses72.
- Java plum or Indian blackberry (also called Jamun or Jambul in Hindi, botanical name Syzygium cumini) effects in-vitro proved to be at par with cromolyn sodium73.
- There are anecdotical mentions of Ephedra sinica (Ma huang) but no clinical trials were conducted 74.
Nutraceuticals for Histamine Degradation
Intestinal histamine can undergo histamine metabolism via gastrointestinal degradation. A clinical trial had proven that supplementation with over-the-counter DAO significantly reduces levels of histamine in digestive tract and improves intolerance symptoms75. Since the positive research results were obtained fairly recently, there is no wide supply of DAO supplements except, maybe, Histamine Block (you can reliably buy it here).
Conclusion
If you think you or your client might have histamine intolerance, conversation with the attending physicians may help to evaluate other possible “look-alike” conditions. Conditions such as true allergies, mastocytosis, or digestive disorders can look similar to histamine intolerance, so they have to be confirmed if possible, and addressed before dealing with histamine intolerance.
At the same time, the Histamine assessment tool offered by Nutri-IQ narrows possibility of histamine intolerance diagnosis, and can render significant help to nutritionists and functional medicine practitioners helping the clients with histamine intolerance.
When the diagnosis is confirmed, it can be followed by therapy based on histamine-free and nutrient-rich diet, lifestyle changes, appropriate prescription, and sufficient supplementation.
References
- Schnedl WJ, Enko D. Considering histamine in functional gastrointestinal disorders. Crit Rev Food Sci Nutr. 2020 Jul 9:1-8. doi: 10.1080/10408398.2020.1791049.
- Western Countries 2020. Downloaded on January 6, 2021
- Tucci, V., & Moukaddam, N. (2017). We are the hollow men: The worldwide epidemic of mental illness, psychiatric and behavioral emergencies, and its impact on patients and providers. Journal of emergencies, trauma, and shock, 10(1), 4–6. https://doi.org/10.4103/0974-2700.199517
- AD. Sperber, SI Bangdiwala, DA Drossman, UC Ghoshal, M Simren, J Tack, WE Whitehead, DL Dumitrascu, X Fang, S Fukudo, J Kellow, E Okeke, EMM Quigley, M Schmulson, P Whorwell, T Archampong, P Adibi, V Andresen, MA Benninga, B Bonaz, S Bor, LB Fernandez, SC Choi, ES Corazziari, C Francisconi, A Hani, L Lazebnik, YY Lee, A Mulak, MM Rahman, J Santos, M Setshedi, AF Syam, S Vanner, RK Wong, A Lopez-Colombo, V Costa, R Dickman, M Kanazawa, AH Keshteli, R Khatun, I Maleki, P Poitras, N Pratap, O Stefanyuk, S Thomson, J Zeevenhooven, OS Palsson, Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study, Gastroenterology, Volume 160, Issue 1, 2021, Pages 99-114.e3,ISSN 0016-5085, https://doi.org/10.1053/j.gastro.2020.04.014.
- Wikipedia. Downloaded on December 14, 2020
- Shirley, David W. PharmD; Sterrett, James PharmD, CDE; Haga, Neal PharmD; Durham, Catherine DNP, FNP The therapeutic versatility of antihistamines, The Nurse Practitioner: February 2020 – Volume 45 – Issue 2 – p 8-21 doi: 10.1097/01.NPR.0000651112.76528.ed
- Potnuri, A.G., Allakonda, L., Appavoo, A. et al. Association of histamine with hypertension-induced cardiac remodeling and reduction of hypertrophy with the histamine-2-receptor antagonist famotidine compared with the beta-blocker metoprolol.Hypertens Res 41, 1023–1035 (2018). https://doi.org/10.1038/s41440-018-0109-2
- The Human Body. Editor(s): Bruce M. Carlson, Academic Press, 2019, ISBN 9780128042540, https://doi.org/10.1016/B978-0-12-804254-0.00008-9
- J Biol Regul Homeost Agents. 2020 Sep-Oct;34(5):1629-1632. doi: 10.23812/20-2EDIT.
- Comas-Basté, O.; Sánchez-Pérez, S.; Veciana-Nogués, M.T.; Latorre-Moratalla, M.; Vidal-Carou, M.d.C. Histamine Intolerance: The Current State of the Art. Biomolecules 2020, 10, 1181.
- What is histamine intolerance? Downloaded on Dec. 16, 2020
- Lieberman P, Garvey LH (2016) Mast cells and anaphylaxis. Curr Allergy Asthma Rep16:20
- Jutel M, Blaser K, Akdis CA. The role of histamine in regulation of immune responses. Chem Immunol Allergy. 2006;91:174-87. doi: 10.1159/000090280. PMID: 16354958.
- Schnedl, W. J., Lackner, S., Enko, D., Schenk, M., Holasek, S. J., & Mangge, H. (2019). Evaluation of symptoms and symptom combinations in histamine intolerance. Intestinal research, 17(3), 427–433. https://doi.org/10.5217/ir.2018.00152
- Litschauer-Poursadrollah M, El-Sayad S, Wantke F, Fellinger C, Jarisch R. Bauchschmerzen, Blähbauch, Diarrhoe: Fruktosemalabsorption, Laktoseintoleranz oder Reizdarmsyndrom? [Abdominal spasms, meteorism, diarrhea: fructose intolerance, lactose intolerance or IBS?]. Wien Med Wochenschr. 2012 Dec;162(23-24):506-12. German. doi: 10.1007/s10354-012-0158-0.
- Beverley Rider. “Hives, Headaches and Heartburn: Heal Your Histamine Hangover”. Summerland Publishing, 2020, ISBN-10: 1732907226
- Evaluation of symptoms and symptom combinations in histamine intolerance. Intest Res. 2019;17(3):427-433. Published online March 7, 2019, DOI: https://doi.org/10.5217/ir.2018.00152
- Kovacova-Hanuskova E, et al. Histamine, histamine intoxication and intolerance. Allergol Immunopathol (Madr). 2015. http://dx.doi.org/10.1016/j.aller.2015.05.001
- Ayyadurai, S., Gibson, A.J., D’Costa, S., Overman, E.L., Sommerville, L.J., Poopal, A.C., Mackey, E., Li, Y. and Moeser, A.J. (2017), Frontline Science: Corticotropin‐releasing factor receptor subtype 1 is a critical modulator of mast cell degranulation and stress‐induced pathophysiology. J Leuk Biol, 102: 1299-1312. https://doi.org/10.1189/jlb.2HI0317-088RR
- Laura Maintz, Natalija Novak, Histamine and histamine intolerance, The American Journal of Clinical Nutrition, Volume 85, Issue 5, May 2007, Pages 1185–1196, https://doi.org/10.1093/ajcn/85.5.1185
- Comas-Basté, Oriol & Latorre-Moratalla, Maria Luz & Sánchez-Pérez, Sònia & Veciana-Nogués, M. Teresa & Vidal-Carou, M. Carmen. (2019). Histamine and Other Biogenic Amines in Food. From Scombroid Poisoning to Histamine Intolerance. 10.5772/intechopen.84333.
- Leitner, R., Zoernpfenning, E., & Missbichler, A. (2014). Evaluation of the inhibitory effect of various drugs / active ingredients on the activity of human diamine oxidase in vitro. Clinical and Translational Allergy, 4(Suppl 3), P23. https://doi.org/10.1186/2045-7022-4-S3-P23
- Food Allergy and Food Intolerance. Downloaded from on Dec. 23, 2020
- MV White, The role of histamine in allergic diseases, Journal of Allergy and Clinical Immunology, Volume 86, Issue 4, Part 2, 1990, Pages 599-605, ISSN 0091-6749, https://doi.org/10.1016/S0091-6749(05)80223-4
- Lin RY, Schwartz LB, Curry A, Pesola GR, Knight RJ, Lee HS, Bakalchuk L, Tenenbaum C, Westfal RE. Histamine and tryptase levels in patients with acute allergic reactions: An emergency department-based study. J Allergy Clin Immunol. 2000 Jul;106(1 Pt 1):65-71. doi: 10.1067/mai.2000.107600.
- Pinzer, TC, Tietz, E, Waldmann, E, Schink, M, Neurath, MF, Zopf, Y. Circadian profiling reveals higher histamine plasma levels and lower diamine oxidase serum activities in 24% of patients with suspected histamine intolerance compared to food allergy and controls. Allergy. 2018; 73: 949‐ 957. https://doi.org/10.1111/all.13361
- Wöhrl, Stefan; Hemmer, Wolfgang; Focke, Margarete; Rappersberger, Klemens; Reinhart Jarisch. Histamine Intolerance-Like Symptoms in Healthy Volunteers after Oral Provocation with Liquid Histamine. Allergy and Asthma Proc; Providence Vol. 25, Iss. 5, (Sep 2004): 305-11.
- How does histamine affect our brain and nervous system? Downloaded on Dec. 17, 2020
- Lieberman P. Histamine, antihistamines, and the central nervous system. Allergy Asthma Proc. 2009 Sep-Oct;30(5):482-6. doi: 10.2500/aap.2009.30.3264
- Eduardo E. Benarroch. Histamine in the CNS. Multiple functions and potential neurologic implications. Neurology Oct 2010, 75 (16) 1472-1479; DOI:10.1212/WNL.0b013e3181f884b1
- Brown RE, Stevens DR, Haas HL. The physiology of brain histamine. Prog Neurobiol. 2001 Apr;63(6):637-72. doi: 10.1016/s0301-0082(00)00039-3. PMID: 11164999.
- Yang, X., Liu, C., Zhang, J., Han, H., Wang, X., Liu, Z., & Xu, Y. (2015). Association of histamine N-methyltransferase Thr105Ile polymorphism with Parkinson’s disease and schizophrenia in Han Chinese: a case-control study. PloS one, 10(3), e0119692. DOI:10.1371/journal.pone.0119692
- Cacabelos R, Torrellas C, Fernández-Novoa L, Aliev G. Neuroimmune Crosstalk in CNS Disorders: The Histamine Connection. Curr Pharm Des. 2016;22(7):819-48. doi: 10.2174/1381612822666151209150954. PMID: 26648474.
- Ajeet Kumar, Shalini Dogra, Chandan Sona, Deepmala Umrao, Mamunur Rashid, Sandeep K Singh, Muhammad Wahajuddin, Prem N Yadav, Chronic histamine 3 receptor antagonism alleviates depression like conditions in mice via modulation of brain-derived neurotrophic factor and hypothalamus-pituitary adrenal axis, Psychoneuroendocrinology, Volume 101, 2019, Pages 128-137, https://doi.org/10.1016/j.psyneuen.2018.11.007
- Joseph P. Vande Griend, Sarah L. Anderson, Histamine-1 receptor antagonism for treatment of insomnia, Journal of the American Pharmacists Association, Volume 52, Issue 6, 2012, Pages e210-e219, ISSN 1544-3191, https://doi.org/10.1331/JAPhA.2012.12051
- Raffaele Falsaperla, Piero Pavone, Stefano Miceli Sopo, Fahad Mahmood, Ferdinando Scalia, Giovanni Corsello, Riccardo Lubrano & Giovanna Vitaliti (2014) Epileptic seizures as a manifestation of cow’s milk allergy: a studied relationship and description of our pediatric experience, Expert Review of Clinical Immunology, 10:12, 1597-1609, DOI: 10.1586/1744666X.2014.977259
- Torrealba, F., Riveros, M. E., Contreras, M., & Valdes, J. L. (2012). Histamine and motivation. Frontiers in systems neuroscience, 6, 51. https://doi.org/10.3389/fnsys.2012.00051
- Obara, I, Telezhkin, V, Alrashdi, I, Chazot, PL. Histamine, histamine receptors, and neuropathic pain relief. Br J Pharmacol. 2020; 177: 580– 599. https://doi.org/10.1111/bph.14696
- Popiolek-Barczyk, K., Łażewska, D., Latacz, G., Olejarz, A., Makuch, W., Stark, H., Kieć-Kononowicz, K., & Mika, J. (2018). Antinociceptive effects of novel histamine H3 and H4 receptor antagonists and their influence on morphine analgesia of neuropathic pain in the mouse. British journal of pharmacology, 175(14), 2897–2910. https://doi.org/10.1111/bph.14185
- Wei, H., Viisanen, H., You, H. J., & Pertovaara, A. (2016). Spinal histamine in attenuation of mechanical hypersensitivity in the spinal nerve ligation‐induced model of experimental neuropathy. European Journal of Pharmacology, 772, 1–10.
- Khalilzadeh, E., Azarpey, F., Hazrati, R., & Vafaei Saiah, G. (2018). Evaluation of different classes of histamine H1 and H2 receptor antagonist effects on neuropathic nociceptive behavior following tibial nerve transection in rats. European Journal of Pharmacology, 834, 221–229. https://doi.org/10.1016/j.ejphar.2018.07.011
- Orazov MR, Radzinskiy VY, Khamoshina MB, et al. Histamine metabolism disorder in pathogenesis of chronic pelvic pain in patients with external genital endometriosis. Patologicheskaia Fiziologiia i Eksperimental’naia Terapiia. 2017 Apr-Jun;61(2):56-60.
- Chiarotti, F., & Venerosi, A. (2020). Epidemiology of Autism Spectrum Disorders: A Review of Worldwide Prevalence Estimates Since 2014. Brain Sciences, 10(5), 274. doi:10.3390/brainsci10050274
- Theoharis C. Theoharides, Julia M. Stewart, Smaro Panagiotidou, Isaac Melamed, Mast cells, brain inflammation and autism, European Journal of Pharmacology, Volume 778, 2016, Pages 96-102, ISSN 0014-2999, https://doi.org/10.1016/j.ejphar.2015.03.086.
- Deiteren, A., De Man, J. G., Pelckmans, P. A., & De Winter, B. Y. (2015). Histamine H4 receptors in the gastrointestinal tract. British journal of pharmacology, 172(5), 1165–1178. https://doi.org/10.1111/bph.12989
- Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol 2012;10:712–21. doi:10.1016/j.cgh.2012.02.029
- Wouters MM, Vicario M, Santos J (2015). “The role of mast cells in functional GI disorders”. Gut. 65 (1): 155–168. doi:10.1136/gutjnl-2015-309151
- Fabisiak, A., Włodarczyk, J., Fabisiak, N., Storr, M., & Fichna, J. (2017). Targeting Histamine Receptors in Irritable Bowel Syndrome: A Critical Appraisal. Journal of neurogastroenterology and motility, 23(3), 341–348. https://doi.org/10.5056/jnm16203
- Wolfgang J. Schnedl, Harald Mangge, Michael Schenk, Dietmar Enko, Non-responsive celiac disease may coincide with additional food intolerance/malabsorption, including histamine intolerance, Medical Hypotheses, 2020, 110404, ISSN 0306-9877, https://doi.org/10.1016/j.mehy.2020.110404.
- Schnedl WJ, Enko D. Considering histamine in functional gastrointestinal disorders. Crit Rev Food Sci Nutr. 2020 Jul 9:1-8. doi: 10.1080/10408398.2020.1791049.
- Nakamura, Y., Ishimaru, K., Shibata, S. et al. Regulation of plasma histamine levels by the mast cell clock and its modulation by stress. Sci Rep 7, 39934 (2017). https://doi.org/10.1038/srep39934
- FAO (Food and Agriculture Organization of the United Nations); WHO (World Health Organization). Histamine in Salmonids. Joint FAO/WHO Literature Review; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241514439.
- Laura Maintz, Natalija Novak, Histamine and histamine intolerance, The American Journal of Clinical Nutrition, Volume 85, Issue 5, May 2007, Pages 1185–1196, https://doi.org/10.1093/ajcn/85.5.1185
- Wagner, N., Dirk, D., Peveling‐Oberhag, A., Reese, I., Rady‐Pizarro, U., Mitzel, H. and Staubach, P. (2017), A Popular myth – low‐histamine diet improves chronic spontaneous urticaria – fact or fiction?. J Eur Acad Dermatol Venereol, 31: 650-655. https://doi.org/10.1111/jdv.13966
- Lackner, S., Malcher, V., Enko, D. et al. Histamine-reduced diet and increase of serum diamine oxidase correlating to diet compliance in histamine intolerance. Eur J Clin Nutr73, 102–104 (2019). https://doi.org/10.1038/s41430-018-0260-5
- Schirone M, Visciano P, Tofalo R, Suzzi G. Histamine Food Poisoning. Handb Exp Pharmacol. 2017;241:217-235. doi: 10.1007/164_2016_54. PMID: 27752845.
- Durak-Dados, A., Michalski, M., & Osek, J. (2020). Histamine and Other Biogenic Amines in Food. Journal of veterinary research, 64(2), 281–288. https://doi.org/10.2478/jvetres-2020-0029
- Miyoshi M, Ueno M, Matsuo M, Hamada Y, Takahashi M, Yamamoto M, Yamamoto I, Mikajiri R, Tabuchi S, Wakida K, Yamanishi M, Hirai M, Usami M. Effect of dietary fatty acid and micronutrient intake/energy ratio on serum diamine oxidase activity in healthy women. Nutrition. 2017 Jul-Aug;39-40:67-70. doi: 10.1016/j.nut.2017.03.004.
- Newsletter from Medical News Today. Downloaded on January 5, 2020
- Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol 2014;11:506-14.
- Which probiotics for histamine intolerance? Downloaded from Probiotic Professionals on Jan. 31, 2021
- Sharma G, Im SH. Probiotics as a Potential Immunomodulating Pharmabiotics in Allergic Diseases: Current Status and Future Prospects. Allergy Asthma Immunol Res. 2018 Nov;10(6):575-590. https://doi.org/10.4168/aair.2018.10.6.575
- Antihistamine. Downloaded on December 23, 2020
- Antihistamines. Downloaded from American Association of Allergy, Asthma, and Immunology on Jan. 4, 2021
- Church M.K. (2016) Allergy, Histamine and Antihistamines. In: Hattori Y., Seifert R. (eds) Histamine and Histamine Receptors in Health and Disease. Handbook of Experimental Pharmacology, vol 241. Springer, Cham. https://doi.org/10.1007/164_2016_85
- Weng, Z., Zhang, B., Asadi, S., Sismanopoulos, N., Butcher, A., Fu, X., Katsarou-Katsari, A., Antoniou, C., & Theoharides, T. C. (2012). Quercetin is more effective than cromolyn in blocking human mast cell cytokine release and inhibits contact dermatitis and photosensitivity in humans. PloS one, 7(3), e33805. https://doi.org/10.1371/journal.pone.0033805
- Chauhan SP, Sheth NR, Suhagia BN (2015) Effect of fruits of Opuntia elatior Mill on mast cell degranulation. J Pharm Bioallied Sci 7(2):156–159. https://doi.org/10.4103/0975-7406.148779
- Minutello K, Gupta V. Cromolyn Sodium. [Updated 2020 Oct 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557473/
- Wikipedia. Cromoglicic acid. Downloaded on Jan 10, 2021
- Vadas P, Perelman B. Activated charcoal forms non-IgE binding complexes with peanut proteins. J Allergy Clin Immunol. 2003 Jul;112(1):175-9. doi: 10.1067/mai.2003.1480.
- Chao-Bin Shen, Yan-Ni Gu, Song Wang, Lan Yu. Astragaloside IV, the major bioactive component of Astragalus membranaceus (Fisch.) Radix, attenuates airway inflammation by modulating Th2 cytokines, STAT6 and ROR-γτ transcription factors in an asthmatic mouse model. The Journal of Immunology May 1, 2019, 202 (1 Supplement) 183.6;
- Asif M. (2011). Health effects of omega-3,6,9 fatty acids: Perilla frutescens is a good example of plant oils. Oriental pharmacy and experimental medicine, 11(1), 51–59. https://doi.org/10.1007/s13596-011-0002-x
- Brito, F.A., Lima, L.A., Ramos, M.F.S., Nakamura, M.J., Cavalher-Machado, S.C., Siani, A.C., Henriques, M.G.M.O., & Sampaio, A.L.F.. (2007). Pharmacological study of anti-allergic activity of Syzygium cumini (L.) Skeels. Brazilian Journal of Medical and Biological Research, 40(1), 105-115. https://dx.doi.org/10.1590/S0100-879X2007000100014
- Yarnell, Eric (2016). Herbs for Eosinophilic, Mast-Cell, and Basophilic Diseases. Alternative and Complementary Therapies, 2016/02/0, doi: 10.1089/act.2015.29038.eya
- Schnedl, W.J., Schenk, M., Lackner, S. et al. Diamine oxidase supplementation improves symptoms in patients with histamine intolerance. Food Sci Biotechnol 28, 1779–1784 (2019). https://doi.org/10.1007/s10068-019-00627-3