Nutritional Imbalances Masking As a Disease
On this page
Major nutritional problems stem from nutritional imbalances of B-group vitamins and other essential nutrients. They can mask as disease, go untreated, and severely damage the health. Nutri-IQ recommends to Wellness Practitioners to check nutritional status with our Nutritional Balance Assessment Tool in order to holistically recognize and close nutritional gaps.
Abstract
Nutritional imbalances may mask themselves as severe diseases. As a result, the disease is getting treated, but without visible results. The doctors blame patients for incompliance, the patients are depressed and frustrated for the lack of results (but not lack of side effects!). One of the most obvious examples is deficiency of vitamin B12 mistaken for COPD in older population (Fimognari FL et al.). No matter what the cause is, the symptoms from anemia are the result of the decreased capacity of the blood to carry oxygen and include fatigue and shortness of breath. In this case, application of “golden standard” corticosteroids for COPD will be not effective and even counterproductive, no matter what the dose is.Bottom line, before diving into fixing complex client’s problems that were not resolved by conventional medicine, let’s try to change the angle of view. It is extremely feasible to know your client nutritional status before proceeding with complex, expensive and may be – again – futile treatment plans.
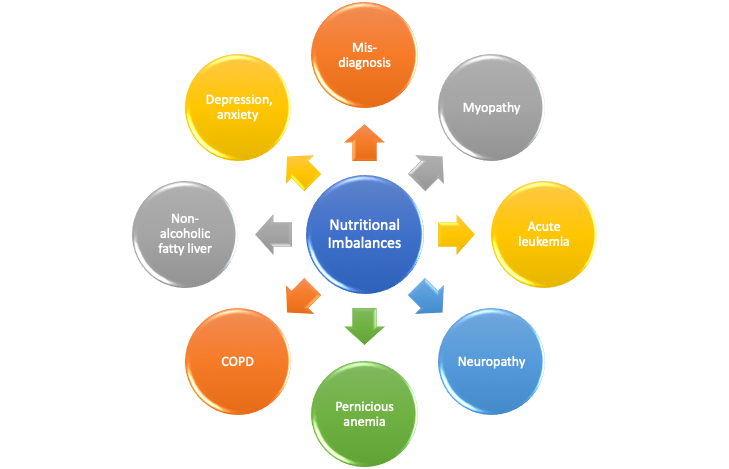
Many Faces of Nutritional Imbalances
Nutritional imbalances may have neurochemical, hormonal and behavioral manifestations and mimic very serious diseases, such as leukemia. Assessment of nutritional balance brings cost-effective immediate answers when your client:
- Feels stressed, tired, depressed
- Takes prescription meds but cannot alleviate symptoms
- Wants to achieve optimal wellness, prevent chronic disease, and manage aging process
Nutri-IQ™ is a unique tool that helps Wellness Professionals to easy and conveniently identify clients’ nutritional gaps as possible causes for clients’ complaints.
Notes:
- As of now, Nutri-IQ tool only deals with manifestations of essential nutrients imbalances. Thus, we focused our efforts on summarizing relevant research results.
- Some published conclusions may have purely anecdotical grounds.
- The results listed below are not exhaustive in terms of imbalance manifestations or symptoms mimicking, and were not compiled to meet any scientific goals.
- Nutri-IQ team did not conduct any research referred here and totally relied upon work conducted by reputable research teams.
Below, we list some major problems associated with nutritional imbalances of B-group vitamins and other essential nutrients. The information is mostly from US Department of Health and Human Services; additional sources and research papers are referenced accordingly.
Vitamin B1 (Thiamin)

People with alcohol dependence; older adults; patients with HIV/AIDS; people with diabetes; and those who underwent geriatric surgery are at risk for thiamin inadequate status. A deficiency leads to decreased activity of thiamine-dependent enzymes that triggers a sequence of metabolic events leading to energy compromise and neuronal death. Thiamin deficiency is more likely to occur can be a contributing factor to heart failure and Alzheimer disease.
Thiamin might play a role in:
- Wernicke-Korsakoff encephalopathy syndrome that in fact may be a Thiamine deficiency (Osiezagha K et al.),
- Diabetes by decreasing glucose levels in patients with type 2 diabetes or impaired glucose tolerance,
- Heart failure improving net change in left ventricular ejection fraction,
- and Alzheimer’s disease as thiamin deficiency might play a role in the development of it.
Vitamin B1 toxicity is rare as the body exerts excess amount with urine.
Vitamin B2 (Riboflavin)

Vitamin B2 deficiency is extremely rare. In addition to inadequate intake, causes of riboflavin deficiency can include endocrine abnormalities (such as thyroid hormone insufficiency) and some diseases. Certain population groups, such as vegetarian athletes; vegans; pregnant and lactating women and their infants; people with infantile Brown-Vialetto-Van Laere syndrome may be at risk because of riboflavin inadequate intake.
Vitamin B2 imbalance mimics mitochondrial myopathy. Riboflavin transporter deficiency is characterized by muscle weakness, ataxia, progressive ponto‐bulbar palsy, amyotrophy, and sensorineural hearing loss (Nimmo et al). Oral riboflavin halts disease progression and may reverse symptoms.
Adverse effects from high riboflavin intakes from foods or supplements (400 mg/day for at least 3 months) have not been reported, but are not deemed impossible.
Vitamin B3 (Niacin)

Severe niacin deficiency leads to pellagra, a disease characterized by a pigmented rash or brown discoloration on skin exposed to sunlight; the skin also develops a roughened, sunburned-like appearance. As pellagra progresses, anorexia develops, and the affected individual eventually dies.
Pellagra causes dementia, diarrhoea, or dermatitis, and can mimic non-specific erythaema in alcoholics. The differential diagnosis between pellagra and non-specific erythaema is important because of the treatability of pellagra by niacin supplementation (Terada N et al).
Niacin inadequacy usually arises from insufficient intakes of foods containing niacin and tryptophan. It can also be caused by factors that reduce the conversion of tryptophan to niacin, such as low intakes of other nutrients. The following groups are among those most likely to have inadequate niacin status: malnourished individuals; people with Hartnup disease; and people with carcinoid syndrome. Despite numerous claims, experts do not agree on the value of nicotinic acid to treat cardiovascular disease, especially given its side effects, safety concerns, and poor patient compliance.
No adverse effects have been reported from the consumption of naturally occurring niacin in foods. However, high intakes of both nicotinic acid and nicotinamide taken as a dietary supplement or medication can cause adverse effects, including hepatotoxicity.
Vitamin B5 (Pantothenic acid)

Because some pantothenic acid is present in almost all foods, deficiency is rare except in people with severe malnutrition. In turn, deficiency of pantothenic acid can mimic depression, fatigue, irritability, and insomnia (Seah 2016). People with a pantothenate kinase-associated neurodegeneration 2 (PKAN) mutation are the most likely group to develop pantothenic acid deficiency.
In terms of health benefits, several clinical trials have shown that the form of pantothenic acid known as pantethine reduces lipid levels when taken in large amounts, but pantothenic acid itself does not appear to have the same effects. Pantothenic acid is very safe, however some individuals taking large doses of pantothenic acid supplements (e.g., 10 g/day) develop mild diarrhea and gastrointestinal distress, but the mechanism for this effect is not known.
Vitamin B6

Isolated vitamin B6 deficiency is uncommon. Inadequate vitamin B6 status is usually associated with low concentrations of other B-complex vitamins, such as vitamin B12 and folic acid. Vitamin B6 deficiency causes biochemical changes that become more obvious as the deficiency progresses. Autoimmune disorders, alcohol dependence, end-stage renal diseases, chronic renal insufficiency, and other kidney diseases can cause vitamin B6 deficiency. In addition, vitamin B6 deficiency can result from malabsorption syndromes, such as celiac disease, Crohn’s disease, and ulcerative colitis. Certain genetic diseases, such as homocystinuria, can also cause vitamin B6 deficiency. Some medications, such as antiepileptic drugs, can lead to deficiency over time.
However, as genetic abnormalities and/or intake or certain medications can cause deficiency of vitamin B6. Its symptoms include anorexia, nausea, listlessness, and lethargy; seborrhea sicca-like dermatitis; cheilosis and conjunctivitis; glossitis; (pellagra-like dermatitis; and polyneuritis (Vilter RW et al). It is worth mentioning that Vitamin B6 deficiency mimics the other B complex deficiency diseases. Research has associated low plasma vitamin B6 concentrations with an increased risk of certain kinds of cancer; cognitive decline; premenstrual syndrome; nausea and vomiting in pregnancy.
High intakes of vitamin B6 from food sources have not been reported to cause adverse effects. However, chronic administration of 1–6 g oral pyridoxine per day for 12–40 months can cause severe and progressive sensory neuropathy characterized by ataxia (loss of control of bodily movements).
Folate (Vitamin B9)

Isolated folate deficiency is uncommon and usually coexists with other nutrient deficiencies because of its strong association with poor diet, alcoholism, and malabsorptive disorders. Megaloblastic anemia is the primary clinical sign of folate or vitamin B12 deficiency.
However, it is not uncommon to get folate deficiency misdiagnosed as more severe conditions. Severe folate deficiency may mimic HELPP syndrome (Gupta RS et al)
Inadequate maternal folate status has been associated with low infant birth weight, preterm delivery, and fetal growth retardation.
The following groups are among those most likely to be at risk of folate inadequacy: people with alcohol use disorder; women of childbearing age; pregnant women; people with malabsorptive disorders; people with the MTHFR polymorphism. Research had shown that inadequate folate status may exist for autism spectrum disorder; cancer (though data about dosage is controversial); cardiovascular disease and stroke; dementia, cognitive function, and Alzheimer’s disease; depression; preterm birth, congenital heart defects, and other congenital anomalies including Neural Tube Disorders.
Concerns have been raised that high folic acid intakes might accelerate the progression of preneoplastic lesions, increasing the risk of colorectal and possibly other cancers in certain individuals. In addition, intakes of 1,000 mcg per day or more of folic acid from supplements during the periconception period have been associated with lower scores on several tests of cognitive development in children at ages 4–5 years than in children of mothers who took 400 mcg to 999 mcg.
Intakes of folic acid that exceed the body’s ability to reduce it to tetrahydrofolate lead to unmetabolized folic acid in the body, which has been linked to reduced numbers and activity of natural killer cells, suggesting that it could affect the immune system. Unmetabolized folic acid might be related to cognitive impairment among older adults.
Vitamin B12 (Cobalamin)

The following groups are among those most likely to be vitamin B12 deficient: older adults; individuals with pernicious anemia, gastrointestinal disorders; people who have had gastrointestinal surgery; vegetarians including pregnant and lactating women who follow strict vegetarian diets and their infants. The main causes of vitamin B12 deficiency include vitamin B12 malabsorption from food, pernicious anemia, postsurgical malabsorption, and dietary deficiency.
Deficiency of Vitamin B12 mimics many diseases.
For instance, it can cause profound alterations in the bone marrow mimicking more serious diagnosis of acute leukemia (Aitelli et al). Vitamin B12-responsive pancytopenia may be misdiagnosed as myelodysplastic syndrome (MDS)(Kim M et al). Symptoms of HELLP syndrome may occur due to vitamin B12 deficiency (Chauvet Eat al). Generalized weakness, weight loss, and progressive pigmentation for suspected Addison’s may be in fact vitamin B12 deficiency (Agrawala RK et al). Pernicious anemia can be associated with autoimmune diseases, such as type 1 diabetes (3% to 4%), vitiligo (2% to 8%), and autoimmune thyroid disease (3% to 32%) (Rodriguez NM et al).
Vitamin B12 deficiency can lead to neurological changes, such as numbness and tingling in the hands and feet, but the neurological symptoms of vitamin B12 deficiency can occur without anemia, so early diagnosis and intervention is important to avoid irreversible damage.
Typically, vitamin B12 deficiency is treated with vitamin B12 injections, since this method bypasses potential barriers to absorption. However, high doses of oral vitamin B12 may also be effective. Overall, an individual patient’s ability to absorb vitamin B12 is the most important factor in determining whether vitamin B12 should be administered orally or via injection.
Large amounts of folic acid can mask the damaging effects of vitamin B12 deficiency by correcting the megaloblastic anemia caused by vitamin B12 deficiency without correcting the neurological damage that also occurs. Moreover, preliminary evidence suggests that high serum folate levels might not only mask vitamin B12 deficiency, but could also exacerbate the anemia and worsen the cognitive symptoms associated with vitamin B12 deficiency.
Biotin

Biotin deficiency is rare. Severe biotin deficiency in healthy individuals eating a normal mixed diet has never been reported. However, the following groups are among those most likely to have inadequate biotin status: individuals with biotinidase deficiency; individuals with chronic alcohol exposure; pregnant and breastfeeding women.
Biotin was promoted for hair, skin, and nail health. Signs of frank biotin deficiency may be observed in individuals with deficiencies in biotin, HLCS gene, and biotinidase, and in individuals consuming large amounts of raw egg white. The biotin-binding protein avidin in raw egg white causes a substantial decrease in the bioavailability of biotin (Janos Zempleni et al).
High biotin intakes may pose another type of health risk. Supplementing with biotin beyond recommended intakes can cause clinically significant falsely high or falsely low laboratory test results, depending on the test. These incorrect results may lead to inappropriate patient management or misdiagnosis of a medical condition.
Choline

Frank choline deficiency in healthy, nonpregnant individuals is very rare, possibly because of the contribution of choline that the body synthesizes endogenously. The following groups are among those most likely to have inadequate choline status: pregnant women; people with genetic alterations; patients requiring total parenteral nutrition; nonalcoholic fatty liver disease sufferers.
Choline deficiency can cause muscle damage, liver damage, and nonalcoholic fatty liver disease (NAFLD or hepatosteatosis).
Despite the hypothesis that choline might affect heart health, several large observational studies have found no significant associations between choline intakes and cardiovascular or peripheral artery disease risk. However, a more recent analysis found an increased risk of mortality in those consuming higher levels of choline. Besides, above-required choline consumption has been shown to increase production of TMAO, a substance that has been linked to a higher risk of cardiovascular disease, in a dose-dependent manner in adults.
Another interesting fact about choline is that the compositions of the gastrointestinal microbial communities changed with choline levels of diets (Spencer MD et al).
People with Alzheimer’s disease have lower levels of the enzyme that converts choline into acetylcholine in the brain.
Vitamin A

Premature infants, pregnant and lactation women, patients with cystic fibrosis, cancer, age-related macular degeneration are at risk for vitamin A deficiency or adverse effects. One of them is night blindness which is in fact reversible if associated with vitamin A deficiency (Clifford LJ et al). There was some research assessing retinoic acid roles in endocrine system (Brossaud J et al) as it is sometimes considered to have hormone-like effects.
Excess preformed vitamin A can have significant toxicity leading to increased intracranial pressure (pseudotumor cerebri), dizziness, nausea, headaches, skin irritation, pain in joints and bones, coma, and even death.
Vitamin C

Vitamin C inadequacy can occur with intakes that fall below the RDA but are above the amount required to prevent overt deficiency (approximately 10 mg/day). The following groups are more likely than others to be at risk of obtaining insufficient amounts of vitamin C: smokers and passive smokers; infants fed evaporated or boiled milk; individuals with limited food variety; people with malabsorption and certain chronic diseases (cachexia and some cancer patients).
Acute vitamin C deficiency leads to scurvy. Today, vitamin C deficiency and scurvy are rare in developed countries but can still occur in people with limited food variety. Overt deficiency symptoms occur only if vitamin C intake falls below approximately 10 mg/day for many weeks.
The timeline for the development of scurvy varies, depending on vitamin C body stores, but signs can appear within 1 month of little or no vitamin C intake. Initial symptoms can include fatigue (probably the result of impaired carnitine biosynthesis), malaise, and inflammation of the gums. As vitamin C deficiency progresses, collagen synthesis becomes impaired and connective tissues become weakened, causing petechiae, ecchymoses, purpura, joint pain, poor wound healing, hyperkeratosis, and corkscrew hairs. Additional signs of scurvy include depression as well as swollen, bleeding gums and loosening or loss of teeth due to tissue and capillary fragility. Iron deficiency anemia can also occur due to increased bleeding and decreased nonheme iron absorption secondary to low vitamin C intake. In children, bone disease can be present. Unfortunately, scurvy can be misdiagnosed as a high-prevalence rheumatoid arthritis (Mertens TM et al).
Left untreated, scurvy is fatal.
Vitamin C has low toxicity and is not believed to cause serious adverse effects at high intakes. The most common complaints are diarrhea, nausea, abdominal cramps, and other gastrointestinal disturbances due to the osmotic effect of unabsorbed vitamin C in the gastrointestinal tract.
Vitamin D

Obtaining sufficient vitamin D from natural food sources alone is difficult. Vitamin D deficiency remains common and may mimic other musculoskeletal disorders or mental health problems requireing harsh interventions, i.e. chemotherapy (BMJ 2008;336:1371).
For many people, consuming vitamin D-fortified foods and, arguably, being exposed to some sunlight are essential for maintaining a healthy vitamin D status. In some groups, dietary supplements might be required to meet the daily need for vitamin D. These groups include breastfed infants; older adults; people with limited sun exposure; individuals with darker skin; people with inflammatory bowel disease and other conditions causing fat malabsorption; people who are obese or who have undergone gastric bypass surgery.
Vitamin D had been shown to provide benefits for osteoporosis. Besides having well‐known control functions of calcium and phosphorus metabolism, bone formation and mineralization, vitamin D also has a role in the maintenance of immune‐homeostasis (Szodoray P et al). Strong biological and mechanistic bases indicate that vitamin D plays a role in the prevention of colon, prostate, and breast cancers. Emerging epidemiologic data suggest that vitamin D may have a protective effect against colon cancer, but the data are not as strong for a protective effect against prostate and breast cancer, and are variable for cancers at other sites.
Vitamin D toxicity can cause non-specific symptoms such as anorexia, weight loss, polyuria, and heart arrhythmias, but also, it can raise blood levels of calcium which leads to vascular and tissue calcification, with subsequent damage to the heart, blood vessels, and kidneys. One study of Finnish smokers, for example, found that subjects in the highest quintile of baseline vitamin D status had a threefold higher risk of developing pancreatic cancer (Buisir BAB).
Vitamin E (Alpha-Tocopherol)

The vast majority of published work has focused on vitamin E’s antioxidant properties. Among other roles, vitamin E has been described as a regulator of signal transduction, gene expression, and redox sensor. The introduction of the free radical theory of brain aging has propelled a renewed interest in this vitamin (Joshi et al).
Frank vitamin E deficiency is rare and overt deficiency symptoms have not been found in healthy people who obtain little vitamin E from their diets. However, it can be mistaken for motor neuropathy (Fusco et al).
Health benefits of alpha-tocoferol were reported for delaying and prevention of coronary heart disease, cancer, eye disorders, and cognitive decline. Research has not found any adverse effects from consuming vitamin E in food. However, high doses of alpha-tocopherol supplements can cause hemorrhage and interrupt blood coagulation in animals.
Research has not found any adverse effects from consuming vitamin E in food. However, high doses of alpha-tocopherol supplements can cause hemorrhage and interrupt blood coagulation in animals, and in vitro data suggest that high doses inhibit platelet aggregation.
Vitamin K

Vitamin K deficiency can occur during the first few weeks of infancy due to low placental transfer of phylloquinone, low clotting factor levels, and low vitamin K content of breast milk. Clinically significant vitamin K deficiency in adults is very rare and is usually limited to people with malabsorption disorders or those taking drugs that interfere with vitamin K metabolism.
Although it is important to consider child abuse when the history and examination substantiate this assumption, it is equally important to consider other potential diagnoses including Vitamin K deficiency (Brousseau TJ et al).
In healthy people consuming a varied diet, achieving a vitamin K intake low enough to alter standard clinical measures of blood coagulation is almost impossible. No adverse effects associated with vitamin K consumption from food or supplements have been reported in humans or animals.
To be continued…
REFERENCES
- 2008, Unrecognised severe vitamin D deficiency. BMJ, and 336:1371.
- Agrawala RK, Sahoo SK, Choudhury AK, Mohanty BK, Baliarsinha AK. Pigmentation in vitamin B12 deficiency masquerading Addison’s pigmentation: A rare presentation. Indian J Endocrinol Metab. 2013, and 17(Suppl 1):S254–S256. doi:10.4103/2230-8210.119591.
- Aitelli, Cristi, et al. “Pernicious anemia: presentations mimicking acute leukemia.” Southern Medical Journal, Mar. 2004, p. 295+. Gale Academic Onefile.
- Brossaud J, Pallet V, Corcuff JB. Vitamin A, endocrine tissues and hormones: interplay and interactions. Endocr Connect. 2017, and 6(7):R121–R130. Published 2017 Aug 9. doi:10.1530/EC-17-0101.
- Brousseau TJ, Kissoon N,McIntosh B. Vitamin K deficiency mimicking child abuse, The Journal of Emergency Medicine,V 29, Issue 3, 2005,p 283-288.
- Bruce N. Ames, The Metabolic Tune-Up: Metabolic Harmony and Disease Prevention, The Journal of Nutrition, Volume 133, Issue 5, May 2003, Pages 1544S–1548S.
- Buisir, BAB Anticancer Effect of Vitamin D Faculty of Basic Medical Science – Libyan International Medical University. 2019, http://repository.limu.edu.ly/handle/123456789/592.
- Chauvet E, Youssef M, Boukhari R, El Guindi W, Carles G. [Symptoms of HELLP syndrome due to vitamin B12 deficiency: report of seven cases]. J Gynecol Obstet Biol Reprod (Paris). 2009 May, and 38(3) 226-230. doi:10.1016/j.jgyn.2009.02.005. PMID: 19304410.
- Clifford LJ, Turnbull AMJ, Denning AM. Reversible night blindness – A reminder of the increasing importance of vitamin A deficiency in the developed world J Optom. 2013, and 6(3):173–174. doi:10.1016/j.optom.2013.01.002.
- Fimognari FL, Loffredo L, Di Simone S, Sampietro F, Pastorelli R, Monaldo M, Violi F, D’Angelo A: Hyperhomocysteinaemia and poor vitamin B status in chronic obstructive pulmonary disease. Nutr Metab Cardiovasc Dis 2009,19(9):654–9.
- Fusco, C., Frattini, D., Pisani, F., Gellera, C., & Giustina, E. D. (2008). Isolated Vitamin E Deficiency Mimicking Distal Hereditary Motor Neuropathy in a 13-Year-Old Boy. Journal of Child Neurology, 23(11), 1328–1330.
- Gupta RS, Rajaram S, Goel N, Singh KC. Severe folate deficiency mimicking HELLP syndrome–report of two cases. J Indian Med Assoc. 2003 Jan, and 101(1) 32-34. PMID: 12841505.
- Janos Zempleni, Toshinobu Kuroishi, Biotin, Advances in Nutrition, Volume 3, Issue 2, March 2012, Pages 213–214.
- Joshi, Y.B. and Praticò, D. (2012), Vitamin E in aging, dementia, and Alzheimer’s disease. BioFactors, 38: 90-97. doi:10.1002/biof.195.
- Kim M, Lee S-E, Park J, Lim J, Cho B-S, Kim Y-J, Kim H-J, Lee S, Min C-K, Kim Y, Cho S-G: Vitamin B12-Responsive Pancytopenia Mimicking Myelodysplastic Syndrome. Acta Haematol 2011, and 125:198-201. doi: 10.1159/000322941.
- Mertens TM, Gertner E. Rheumatic Manifestations of Scurvy: A Report of Three Recent Cases in a Major Urban Center and a Review. Seminars in Arthritis and Rheumatism,V 41, Issue 2, 2011,p 286-290.
- Nimmo, GAM, Ejaz, R, Cordeiro, D, Kannu, P, Mercimek‐Andrews, S. Riboflavin transporter deficiency mimicking mitochondrial myopathy caused by complex II deficiency. Am J Med Genet Part A. 2018, and 176A: 399– 403.
- 2020. Nutri-IQ™, unique tool that helps Wellness Professionals to easy and conveniently identify clients’ nutritional gaps as possible causes for clients’ complaints. https://www.nutriiq.ca.
- Osiezagha K, Ali S, Freeman C, et al. Thiamine deficiency and delirium. Innov Clin Neurosci. 2013, and 10(4):26–32.
- Rodriguez NM, Shackelford KS. Pernicious Anemia. [Updated 2019 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, and 2019 Jan-.
- Seah, Siew Ling. 2016. “Food and Mental Health.” Sinapore: Partridge Publishing, August 12.
- Spencer MD, Hamp TJ, Reid RW, Fischer LM, Zeisel SH, Fodor AA.Association Between Composition of the Human Gastrointestinal Microbiome and Development of Fatty Liver With Choline Deficiency. Gastroenterology,V 140, Issue 3, 2011,p 976-986.
- Szodoray P, Nakken B, Gaal J, Jonsson R, Szegedi A, Zold E, Szegedi G, Brun J,G, Gesztelyi R, Zeher M, Bodolay E (2008). The Complex Role of Vitamin D in Autoimmune Diseases, Scandinavian Journal of Immunology 68: 261-269.
- Terada N, Kinoshita K, Taguchi S, et al Wernicke encephalopathy and pellagra in an alcoholic and malnourished patient Case Reports 2015, and 2015:bcr2015209412.
- US Department of Health and Human Services. https://ods.od.nih.gov.
- Vilter RW et al. The effect of vitamin B6 deficiency induced by desoxypyridoxine in human beings. The Journal of Laboratory and Clinical Medicine, Volume 42, Issue 3, 335 – 357.